本期为Worldneurosurgery定期连载的河南省人民医院张长远医师终审的《动脉瘤大师级神作--Seven Aneurysms》著作第六期。本期主要内容为 永久夹闭,《Seven Aneurysms 》系列内容包括 Section I The Tenets:1. 在显微镜下操作;2. 蛛网膜下腔的解剖;3.脑牵拉;4.血管控制;5.临时夹闭;6.永久夹闭;7.检测;8.脑皮层造瘘;9.术中破裂。Section II The Approaches: 10.翼点入路; 11.眶颧入路; 12.前纵裂入路; 13.远外侧入路。Section IIIThe Seven Aneurysms: 14.后交通动脉瘤; 15.大脑中动脉瘤; 16.前交通动脉瘤; 17.眼动脉动脉瘤; 18.胼周动脉瘤; 19.基底动脉分叉动脉瘤; 20.小脑后下动脉动脉瘤。
【Seven Aneurysms】往期回顾
第六期:Permanent Clipping--永久夹闭
■ Clip Application--动脉瘤夹的应用
Applying a permanent clip on an aneurysm neck is like land-ing an airplane, requiring just the right “yaw, pitch, and roll” (Fig. 6.1A). Pitch refers to the slope of the clip appliers; yaw refers to the side-to-side rotation of the clip appliers about a vertical axis; and roll refers to the side-to-side rotation of the clip appliers about the instrument’s axis. Adjustments are made by the wrist while the hand and fingers stabilize the appliers, squeeze it to open the clip blades, and gently release pressure when the clip is in position. With small, sessile aneurysms, downward pressure may also be required as the clip is released.
在动脉瘤瘤颈部使用放置永久夹就像驾驶飞机着陆,需要恰当正确的“转向偏转,俯仰和滚动自旋角”(图6.1A)。俯仰是指施夹器的斜度;转向偏转是指施夹器围绕竖纵轴的旋转; 滚动自旋是指围绕沿施夹器长轴的轴向转动。当手和手指稳定住施夹器时,调整角度靠手腕进行,捏施夹器以打开叶片,当夹子调整至理想位置后轻轻释放压力。对于小的、宽基底的动脉瘤,随着阻断夹的释放,可能需要向下的压力。
Permanent clip application demands complete visual-ization from start to finish, from the introduction of perma-nent clips into the field to their release from the appliers. Both sides of the aneurysm neck, both clip blades, and the adjacent anatomy are brought into one panoramic view by shifting the microscope, decreasing the zoom, and adjusting retractors. Clip appliers obstruct an established line of sight if they enter the surgical corridor along or near the line of sight; a 15- to 30-degree difference between the appliers’ line and the sight line is needed to visualize the blades on the aneurysm neck ( Fig. 6.1B). The appliers’ line is often fixed by the aneurysm anatomy, which requires shifting the microscope to offset the sight line. Clip application should not proceed without complete visualization.
应用放置永久夹的过程--从永久夹进入术野到从施夹器释放,自始至终需要完全看清楚。通过移动显微镜、降低放大倍数和调整牵开器的位置,使动脉瘤颈两侧,夹子的两个叶片和相邻的解剖结构均进入包含在一个视野中。如果施夹器沿着或接近视线的方向进入手术通道,施夹器会阻挡视线. 需要在施夹器轴线与术者视线间调整15°到30°度以看清动脉瘤颈瘤夹两侧的叶片(图6.1B)。由于动脉瘤的解剖限制,施夹器的轴线常是不能变的,这就需要移动显微镜以调整视线。在没有获得完整视野之前,不应该释放动脉瘤夹。
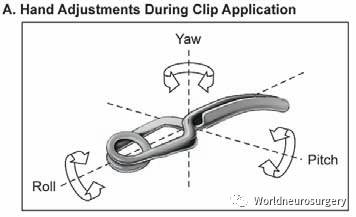
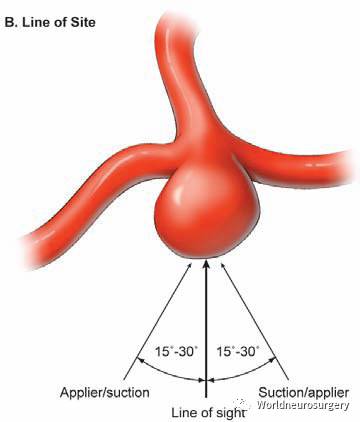
Fig. 6.1 (A) Clip application requires adjusting the yaw, pitch, and roll of the clip. Pitch refers to the slope of the clip appliers; yaw refers to the side-to-side rotation of the clip appliers about a vertical axis; and roll refers to the side-to-side rotation of the clip appliers about the instrument’s axis. (B) Permanent clip application demands complete visualization of the aneurysm neck, both clip blades, and adjacent anatomy. A line of sight is established that brings these together in one panoramic view. The working line of the clip appliers must be 15 to 30 degrees off of the sight line of the microscope to preserve the view. The appliers’ line is often fixed by aneurysm anatomy, which requires shifting the microscope to offset the sight line.
图.6.1(A)放置永久夹需要调整动脉瘤夹的偏转,俯仰和自旋角。俯仰是指施夹器的斜度;转向偏转是指施夹器围绕竖纵轴的旋转; 滚动自旋是指围绕沿施夹器长轴的轴向转动。(B)放置永久动脉瘤夹需要完全看清楚动脉瘤颈、瘤夹的两个叶片和相邻的解剖结构。让这些结构完全包含在一个视野里。施夹器的工作轴向必须偏离显微镜的视轴线15°到30°度以保证视野清楚。由于动脉瘤的解剖限制,施夹器的轴线常是不能变的,这就需要移动显微镜以调整视线。
Rhoton introduced four rules about aneurysms: aneu-rysms arise at branching sites on the parent artery, which may be a side branch or a bifurcation (rule 1); aneurysms arise at turns or curves in the outer wall of the artery where hemodynamic stress is greatest (rule 2); aneurysms point
in the direction that blood would have gone if the curve at the aneurysm site was not present (rule 3); and each aneurysm is associated with a set of perforating arteries that needs to be preserved (rule 4). According to rule 1, the clip should be applied perpendicular to the afferent artery and parallel to the efferent branches with bifurcation aneurysms (e.g., middle cerebral artery [MCA] and basilar bifurcation aneurysms). According to rules 2 and 3, the clip is applied
parallel to the parent artery with aneurysms at curves (e.g., ophthalmic artery [OphA] and superior hypophyseal artery [SHA] aneurysms). According to rule 4, the clip is applied par-allel to the line of perforators across an aneurysm base (e.g., anterior communicating artery [ACoA] and basilar bifurca-tion aneurysms). Not every aneurysm conforms to Rhoton’s rules, but analyzing aneurysm anatomy from this perspec-tive helps envision the repair and select appropriate clips.
Rhoton提出了关于动脉瘤的四条法则:动脉瘤发生在载瘤动脉的分岔点,可能是侧支或分叉处(法则1);动脉瘤发生在血流动力学应力最大的动脉转折或弯曲处的外壁(法则2);如果动脉瘤处没有弯曲,则动脉瘤指向与血流的方向一致(法则3);每个动脉瘤都与一组需要保护的穿支动脉有关(法则4)。根据法则1,对于分岔处动脉瘤,动脉瘤夹应垂直于流入动脉并平行于流出动脉分支(例如,大脑中动脉和基底动脉分岔处动脉瘤)。根据法则2和3,对于弯曲处动脉瘤,动脉瘤夹应平行于载瘤动脉(例如,眼动脉[OphA]和垂体上动脉[SHA]动脉瘤)。根据法则4,动脉瘤夹应放置在平行于穿支的跨动脉瘤基底处(例如,前交通动脉[ACoA]和基底动脉分叉处动脉瘤)。并不是每个动脉瘤都符合Rhoton法则,但是从这个角度分析动脉瘤解剖,有助于设定方案并选择合适的动脉瘤夹。
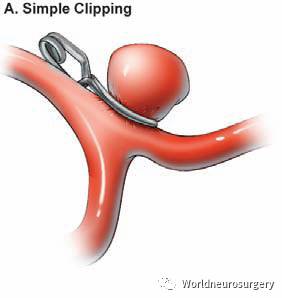
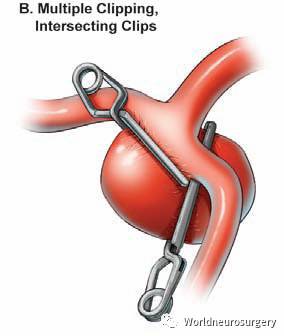
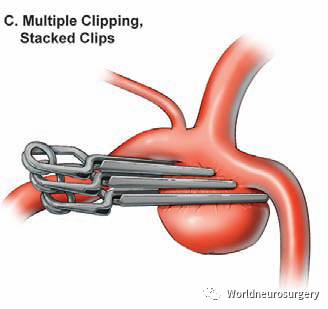
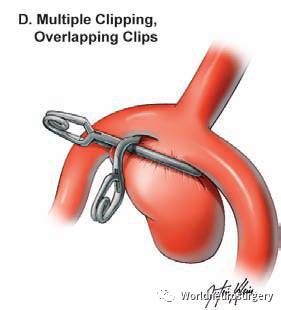
Fig. 6.2 Basic clipping techniques. (A) Simple clipping with a single clip. (B) Multiple clipping with intersecting clips. (C) Multiple clipping with parallel stacked clips. (D) Multiple clipping with an overlapping fenestrated clip closing the posterior lobe of aneurysm.
图. 6.2基本夹闭技术。(A)使用单个动脉瘤夹的简单夹闭。(B)用交叉动脉瘤夹行多重夹闭。 (C)用平行层叠动脉瘤夹的多重夹闭。(D)叠加一个窗夹夹闭动脉瘤后叶的多重夹闭。
■ Simple Clipping--简单夹闭
A basic rule of aneurysm clipping is “simple is best.” Simple clipping uses a single clip, usually with aneurysms that are small, have narrow necks, and uncomplicated anatomy ( Fig. 6.2A). Reliance on a single clip requires the perfect clip size, contour, and configuration. The part of the blade that matters is the part that crosses the neck. Small, deep aneu-rysms in tight surgical corridors, such as at the basilar apex, may still require long clip blades that move back the clip’s coiled spring and keep the head of the appliers from ob-structing the line of sight.
动脉瘤夹闭的基本原则是“简单最好”。简单夹闭使用单个瘤夹,通常用于小的,窄颈,解剖不复杂的动脉瘤(图6.2A)。值得信赖的单个瘤夹需要有完美的大小,轮廓和结构。叶片重要的部分是跨瘤颈的部分。狭窄的手术通道(例如基底动脉尖处)里的小的、深在的动脉瘤可能仍然需要长叶片瘤夹,以便能后移瘤夹的弹簧,保证施夹器的头部不会阻挡视线。
■ Multiple Clipping--多重夹闭
Simple clipping may not be possible with aneurysms that are large, have broad necks, and complex anatomy. These aneurysms require multiple clips, which close an aneurysm neck in sequential steps, progressing from deep neck to near neck and tackling the most difficult, inaccessible part first. Multiple clips can contour the neck reconstruction to match the anatomy of the neck and efferent arteries. Multiple clip-ping strategies are common and include intersecting clips, stacked clips, and overlapping clips.
对于大的、宽颈、解剖复杂的动脉瘤可能无法进行简单的夹闭。这些动脉瘤需要多个瘤夹分步骤依次进行动脉瘤颈夹闭,逐步从颈深部至颈浅部,首先解决最困难、最难以接近的部分。多个瘤夹可以重建瘤颈的轮廓以适应瘤颈的解剖和流出动脉。多重夹闭的策略很常见,包括交叉瘤夹、层叠瘤夹和交叠瘤夹。
Multiple clipping with intersecting clips uses a second clip angled into an initial clip, with its tips intersecting the blade or heel of the initial clip at an acute, right, or obtuse angle (Fig. 6.2B ). Intersecting clips can be simple, such as two straight clips in a T-configuration, or complex, such as mul-tiple straight clips that converge like leaves of a camera’s aperture. Stacked clips are applied parallel to each other ( Fig. 6.2C). The initial clip typically closes most of the aneurysm,
and tips of subsequent clips precisely contour the remnant beneath the initial clip (understacking) . When the initial clip is applied near the neck but does not adequately reconstruct it, subsequent clips stacked above it will complete the clo-sure (overstacking). Stacked clips are all applied in the same direction, which facilitates clipping in tight surgical corridors where the appliers cannot be maneuvered to intersecting angles. Understacking precisely contours the origins of ef-ferent arteries as they exit the aneurysm’s base, and under-stacking with mini-clips eliminates tiny dog-ear remnants. An overlapping fenestrated clip can be applied over an initial straight clip at various angles to close a distal neck remnant beneath the initial clip ( Fig. 6.2D). This overlapping clip reconstruction encircles the initial clip blade, bringing the heel of the fenestrated clip blade against the straight clip blade.
交叉瘤夹的多重夹闭是用第二个瘤夹与第一个瘤夹成角度进入,其尖端与第一个瘤夹的叶片或根部交叉成锐角、直角或钝角(图6.2B)。交叉瘤夹可以简单,例如两个直夹呈T形结构,也可以复杂,例如多个直夹像相机光圈的叶片那样会聚。层叠瘤夹彼此平行(图6.2C)。第一个瘤夹通常夹闭动脉瘤的大部分,后续瘤夹的尖端在第一个瘤夹之下(下层叠)精确地夹闭动脉瘤残余。当第一个瘤夹接近瘤颈但不能完全重建时,随后的瘤夹层叠其上完成夹闭(上层叠)。层叠瘤夹都方向相同,这有助于术者在无法交叉夹闭的不宽裕的手术通道中完成夹闭。下层叠精确地勾勒出流出动脉发自动脉瘤基底的起源,且使用微型瘤夹的下层叠技术可消除小的狗耳朵状残留。交叠开窗夹可以以多种角度越过第一个直夹,以在第一个瘤夹下方夹闭远端的瘤颈残余(图6.2D)。这个交叠的瘤夹围绕着第一个瘤夹的叶片进行重建,使得开窗夹叶片的根部抵着直夹的叶片。
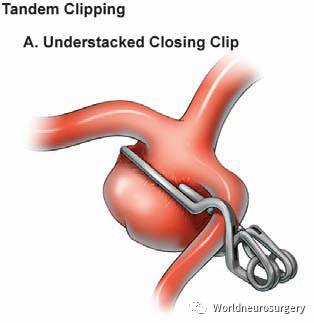
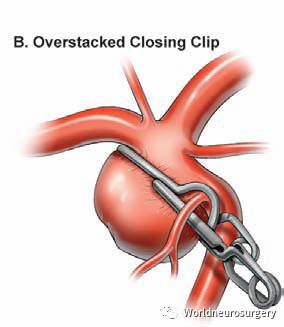
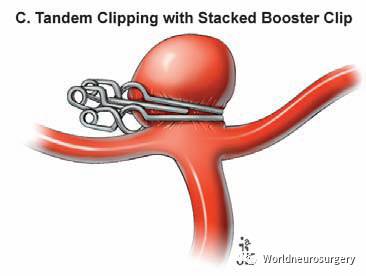
Fig. 6.3 Tandem clipping techniques. (A) Tandem clipping with an understacked closing clip. (B) Tandem clipping with an overstacked closing clip. (C) Tandem clipping with an overstacked closing clip and a stacked fenestrated booster clip to reinforce the closure at the distal neck.
图.6.3串联夹闭技术。(A)使用下层叠无窗瘤夹进行串联夹闭。(B)使用上层叠无窗瘤夹进行串联夹闭。(C)串联使用上层叠无窗瘤夹夹闭,并用开窗加强夹来强化瘤颈远端的夹闭。
■ Tandem Clipping--串联夹闭
Tandem clipping is a technique developed by Drake that uses a straight fenestrated clip to first close the distal aneurysm neck, and then shorter, simple clips to close the proximal neck encircled by the fenestration (Fig. 6.3). This ingenious technique effectively closes larger aneurysm necks because the closing force of fenestrated clips is maintained distally near their tips. This clip gathers aneurysm tissue and col-lapses the neck to visualize deep anatomy. The shorter clips used to close the fenestration contour the reconstruction of the near neck and preserve efferent arteries there. Tandem clipping with an understacked clip closes the aneurysm neck below the fenestration, and tandem clipping with an over-stacked clip closes the aneurysm neck above the fenestration. Tandem clipping with fenestrated clips is superior to simple clipping with longer clips because longer clips can splay at the tips and allow the aneurysm to refill.
串联夹闭是由 Drake 提出的一种技术,该技术使用直的开窗夹,首先夹闭动脉瘤瘤颈远端,然后使用较短的简单的瘤夹夹闭由开窗围绕的瘤颈近端(图6.3)。这种巧妙的技术可有效地夹闭更大的动脉瘤瘤颈,因为开窗夹的闭合力维持在远端,靠近其尖端。该瘤夹可收拢动脉瘤组织并使瘤颈塌陷,以看清深部解剖。较短的瘤夹用于夹闭开窗部分旷置的近端瘤颈,并保留流出动脉。使用下层叠夹的串联夹闭可闭合开窗下方的动脉瘤瘤颈,使用上层叠夹的串联夹闭可闭合开窗上方的动脉瘤瘤颈。使用开窗夹的串联夹闭优于使用较长阻断夹的简单夹闭,因为较长阻断夹的尖端可能张开,使动脉瘤再次充盈。
■ Tandem Angled Fenestrated Clipping--成角开窗串联夹闭
Tandem angled fenestrated clipping is a technique developed by Sugita that uses multiple angled fenestrated clips applied sequentially across a broad neck projecting away from the
neurosurgeon, as in many paraclinoid internal carotid artery (ICA) aneurysms ( Fig. 6.4 ). This technique typically uses 90-degree angled clips with large fenestrations and blades of varying lengths, curves, and deviations. The clips are aligned with the blade tips in the same direction, and applied toe to heel, progressing from deep neck to near neck. Tandem counterclipping techniques align the blade tips in opposite directions, and can be applied toe to toe (facing) or heel to heel ( cross-wise ). Tandem angled fenestrated clips should overlap at their interface with the adjacent clip; clips that simply meet at their interface may permit the aneurysm to
refill at these points.
成角开窗串联夹闭是由 Sugita 提出的一种技术,该技术使用多个成角的开窗夹,依次跨过指向离开术者的宽的瘤颈,见于许多床突旁颈内动脉(ICA)动脉瘤中(图6.4)。这种技术通常使用大开窗的具有不同长度、曲度和偏角叶片的90度角瘤夹。瘤夹呈一排,叶片尖端呈同一方向,头尾相接,从远端瘤颈依次排到近端瘤颈。相向串联技术时叶片尖端方向相反排列,可头对头(面对面)或脚对脚(交叉状)。成角开窗串联瘤夹应在相邻瘤夹的交界处重叠; 在此处瘤夹仅简单的会合可能造成动脉瘤在这些部位再次充盈。
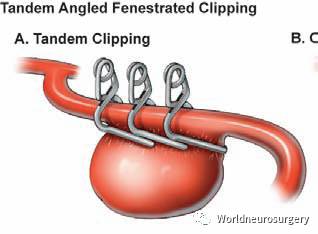
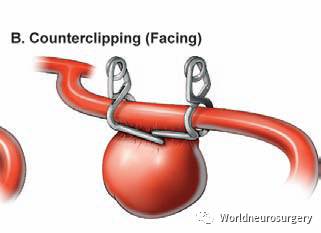
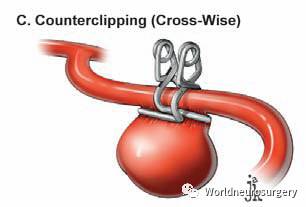
Fig. 6.4 Tandem angled fenestrated clipping. (A) Tandem angled fenestrated clipping with right-angled fenestrated clips placed heel to toe, all in the same direction. (B) Counterclipping with facing right-angled fenestrated clips placed toe to toe (facing). (C) Counterclip-ping with crossing right-angled fenestrated clips placed heel to heel(cross-wise).
图.6.4成角开窗串联夹闭。(A)使用直角开窗夹的成角开窗串联夹闭,均在同一方向脚对头的放置。(B)使用直角开窗夹尖端对尖端、面对面的放置,为相向夹闭。(C)使用交叉直角开窗夹相向夹闭,脚对脚(交叉状)的放置。
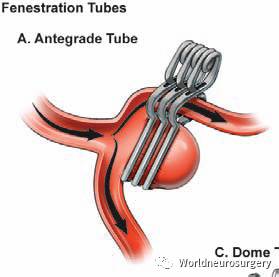
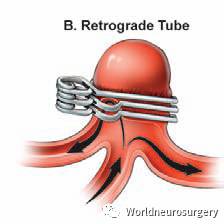
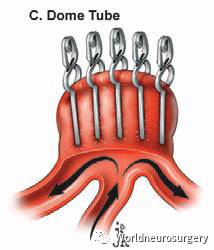
Fig. 6.5 Clipping techniques with fenestration tubes. (A) Antegrade fenestration tube with stacked straight fenestrated clips transmitting an efferent artery with flow antegrade through the tube. (B) Retro-grade fenestration tube with stacked straight fenestrated clips trans-mitting an efferent artery with flow retrograde through the tube. (C) Dome fenestration tube with stacked straight fenestrated clips over the aneurysm dome with the tips reconstructing and contouring
the neck.
图.6.5开窗管的夹闭技术。(A)使用层叠的开窗直夹形成顺行开窗管,使流出动脉以顺行血流通过开窗管。(B)使用层叠的开窗直夹形成逆行开窗管,使流出动脉以逆行血流通过开窗管。C)使用层叠的开窗直夹在动脉瘤瘤顶上形成瘤顶开窗管,用其尖部进行瘤颈塑形夹闭,重建血管。
■ Fenestration Tubes--开窗管
Straight fenestrated clips can be stacked to close an aneu-rysm neck and create a tube that reconstructs an efferent artery. These fenestration tubes can be built in three configu-rations named for the direction of blood flow in the tube (an-tegrade or retrograde), or the part of the occluded aneurysm in the tube (dome) (Fig. 6.5). An antegrade fenestration tube builds an open tube oriented perpendicular to the blades and transmits blood flow through the tube antegrade to the efferent artery. A retrograde fenestration tube builds a closed tube that turns around its blood flow and redirects it to an efferent artery coursing from the aneurysm’s base. A dome fenestration tube does not transmit an efferent artery and instead fenestrates the aneurysm dome. The dome tube is built with stacked straight fenestrated clips perpendicular to the aneurysm neck (rather than parallel to the neck as with other constructs), enabling the tips rather than lengths of the blades to reconstruct the neck. Clipping with fenestration tubes is another microsurgical technique that can be used to treat aneurysms with large or giant size, efferent arteries that adhere to the aneurysm, or unusual branch anatomy.
直的开窗夹可以层叠夹闭动脉瘤瘤颈并重建一条流出动脉的管道。这些开窗管可以有三种结构,按照管中血流方向(顺行或逆行)或管中阻断的动脉瘤的部分(瘤顶)命名(图6.5)。顺行开窗管中管是开放的,方向垂直于叶片,通过该管血顺行流到流出动脉。逆行开窗管中,管的一端是闭合的,血流在此转向,沿动脉瘤根部到流出动脉。瘤顶开窗管并没有流出动脉过渡,而是在动脉瘤瘤顶开窗。瘤顶管是用垂直于动脉瘤瘤颈的层叠的开窗直夹(而不是像其他结构那样平行于瘤颈)构成的,用瘤夹尖端而非叶片重建瘤颈。开窗管夹闭是另一种显微外科技术,可用于治疗大型或巨大型动脉瘤、流出动脉粘附于动脉瘤或分支解剖异常的动脉瘤。
■ Clip Reconstruction--动脉瘤夹重建
Permanent clipping sometimes requires deliberately enter-ing an aneurysm. The neck of a thrombotic aneurysm can be softened with thrombectomy; the neck of a recurrent aneu-rysm with coil compaction can be softened by mobilizing coils out of the blade pathway; the clipping of some giant aneurysms can be simplified by decapitating the aneurysm. These maneuvers leave a gaping hole in the aneurysm and require a reconstructive repair ( Fig. 6.6). Techniques for clip reconstruction are selected from the same menu as other aneurysms, but clip reconstruction can be more difficult for the following reasons: incomplete proximal and distal con-trol with back-bleeding; adherent perforators and branch ar-teries that require mobilization; difficulty in reconstructing a neck after transecting the aneurysm; and atherosclerotic tissue at the neck. These reconstructions are performed under the pressure of ongoing ischemia. Unexpected prob-lems must be solved quickly because the brain can be reperfused only after an opened aneurysm has been closed completely. Therefore, opening an aneurysm may facilitate its occlusion and appeals to the neurosurgeon’s instinct to attack the aneurysm directly, but it is fraught with uncer-tainty, tension, and risk. Thrombectomy works best when only a limited debulking is necessary. Concentric thrombotic aneurysms with thin layers of thrombus at the neck require only modest thrombectomy to soften and clip the aneurysm. The same may be true with lobulated and coiled thrombotic aneurysms. Eccentric thrombotic aneurysms with clippable necks may still require thrombectomy to slacken the aneurysm fundus, enable the clips to close the neck, and prevent their migration onto the parent arteries.
永久性夹闭有时需要特意进入动脉瘤。血栓性动脉瘤的瘤颈可以用血栓切除术来变软;弹簧圈填塞的复发性动脉瘤的瘤颈可以将瘤夹叶片通过的地方的弹簧圈去除而变软;巨大动脉瘤的夹闭可以通过切除动脉瘤顶部而变简单。这些操作在动脉瘤中留下一个敞开的洞,需要重建修复(图6.6)。用于夹闭重建的技术从与其他动脉瘤相同的方案中选择,但由于以下原因,夹闭重建可能更困难:用于夹闭重建的技术从与其他动脉瘤相同的方案中选择,但由于以下原因,夹闭重建可能更困难:因近端和远端不完全控制而有血液返流;粘连的穿支动脉和分支动脉需要移动;动脉瘤剖开后的瘤颈重建困难;和瘤颈处有粥样硬化组织。这些重建在持续缺血的压力下进行。必须快速解决意想不到的问题,因为只有在开放的动脉瘤完全闭合后大脑才能进行再灌注。因此,开放动脉瘤可能有助于其闭塞并有助于神经外科医生直觉上能直接处理动脉瘤,但是充满不确定性、紧张感和风险。当只需要有限的减瘤时血栓切除效果才最好。在瘤颈有薄层血栓的同心血栓性动脉瘤只需要适度的血栓切除来软化和夹闭动脉瘤。分叶的和栓塞后血栓性动脉瘤也是如此。瘤颈可夹闭的偏心性血栓性动脉瘤可能仍然需要血栓切除以松弛动脉瘤基底,使瘤夹能够闭合瘤颈,并防止其滑动至载瘤动脉上。
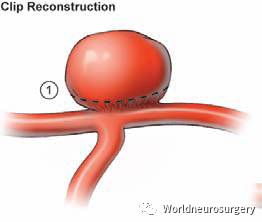
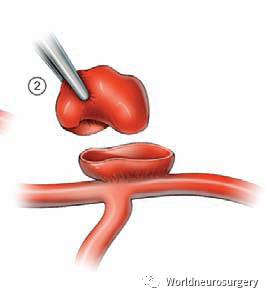
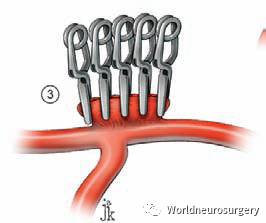
Fig. 6.6 Clip reconstruction technique. (1) The fundus of an un-clippable aneurysm is transected (dashed line ). (2) The aneurysm is opened and it neck is simplified. (3) The neck is then reconstructed and contoured with stacked straight clips, in this case applied perpen-dicular to the aneurysm neck.
图. 6.6夹闭重建技术。(1)切除无法夹闭动脉瘤的基底(虚线)。(2)动脉瘤开放,瘤颈简化。(3)然后用层叠的直夹将瘤颈重建和成形,在这种情况下使用垂直于动脉瘤瘤颈的瘤夹。
编译者:冯刚,深圳大学总医院,神经外科,硕士。
审校1:九江市第一人民医院,神经外科,胡炜,主任医师,医学博士。
审校2:九江市第一人民医院,神经外科,杨枫,主任医师。
终审:河南省人民医院,神经外科,张长远。
【Seven Aneurysms】往期回顾
属于神外医生的宝库!了解 Worldneurosurgery 的8大宝
神外专业手机微官网,识别二维码收藏



点击下方“阅读原文”查看手机微官网
↓↓↓








