
桡动脉介入治疗(transradial intervention,TRI)具有术后不需限制活动、缩短住院时间、患者接受程度高等优点。由泰尔茂公司全力协办的“介入心声音”——第九届年度精彩TRI病例大赛于中国心脏大会(CHC 2017)期间已决出中国区四强,四强选手病例受邀前往日本2017复杂心血管治疗学大会(Complex Catheter Therapeutics,CCT),在“中日TRI病例竞赛”现场展开激烈角逐。本届TRI病例大赛总冠军将花落谁家?敬请期待10月27日《门诊》前方记者于日本CCT现场为您带来盛况报道!

来自中国医学科学院阜外医院崔成医师凭借一例左主干分叉合并严重钙化迂曲的精彩病例荣获一等奖。该患者SYNTAX评分为46,崔医师采用LAD-LM冠状动脉旋磨术结合IVUS影像指导在左主干分叉处成功置入支架。接下来将详细呈现患者的病例资料与医师手术过程,以期各位专家学者交流学习。
General information(Male, 51 years)
Chief complaint: Chest pain 10 yrs, aggravate 1 month.
Past medical history: Previous MI or revascularization: No; Comorbidities: Atrial fibrillation, gastric ulcer, pulmonary interstitial fibrosis.
Risk Factors: Current Smoking 20 years,Diabetes 40 years,Hyperlipidemia 40 years,Hypertension 10 years,PAD 2 years.
Clinical Presentation: Effort and Spontaneous Angina (Braunwald ⅡB) . Echo: LV 49 mm, EF 65 %.
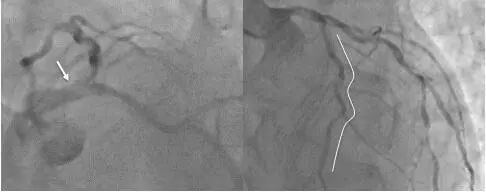
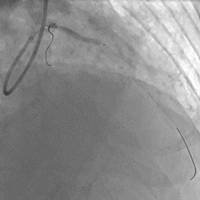
Coronary Angiography
Anatomic Characteristics: LM + Three vessel disease;LM bifurcation disease with severe calcification;LAD diffuse, tortuous & severe calcified disease.
1.SYNTAX Score = 46; 2.SYNTAX Score II CABG = 54.3, PCI 4 Year Mortality = 41.9%; 3.SYNTAX Score II PCI = 55.1, CABG 4 Year Mortality = 43.5%.
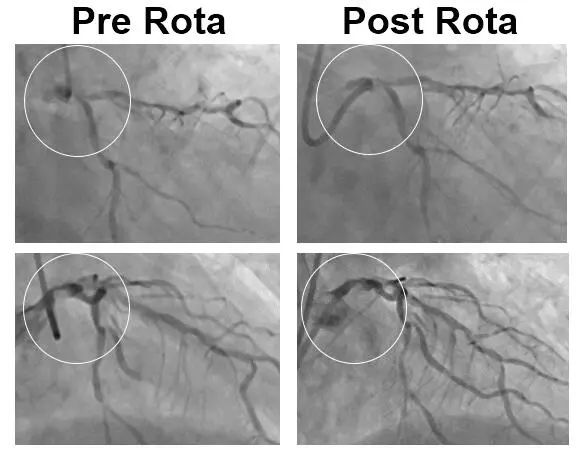
Strategy Selection: 1.CABG recommended but rejected by patient; 2.LCA PCI first, stage PCI for RCA; 3.LAD-LM rotational atherectomy, 1.25 Burr start, From proximal LAD to LM; 4.IVUS evaluation; 5.Provisional stenting for left main bifurcation.
Percutaneous Coronary Intervention
Setp 1: 1.25 mm Burr Rota.

Setp 2: 1.5 mm Burr Rota.

Setp 3: 2.5×15 mm non-compliant balloon.
Setp 4: DES 2.75×22 mm;
DES 3.5×18 mm.

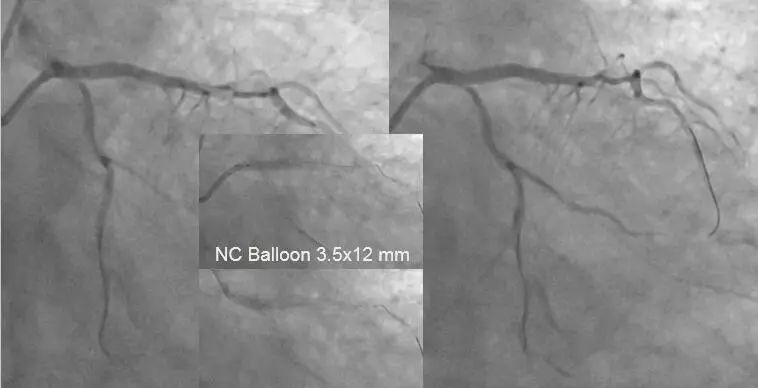
Setp 5: NC balloon 3.5×12mm+2.5×15 mm.
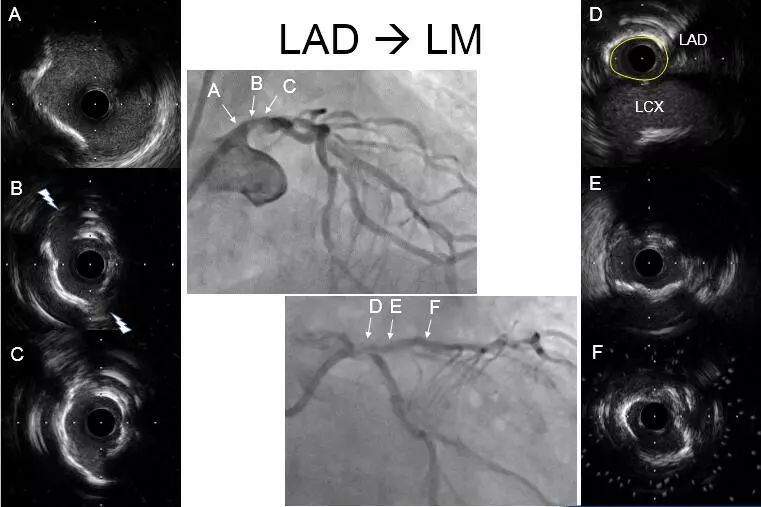
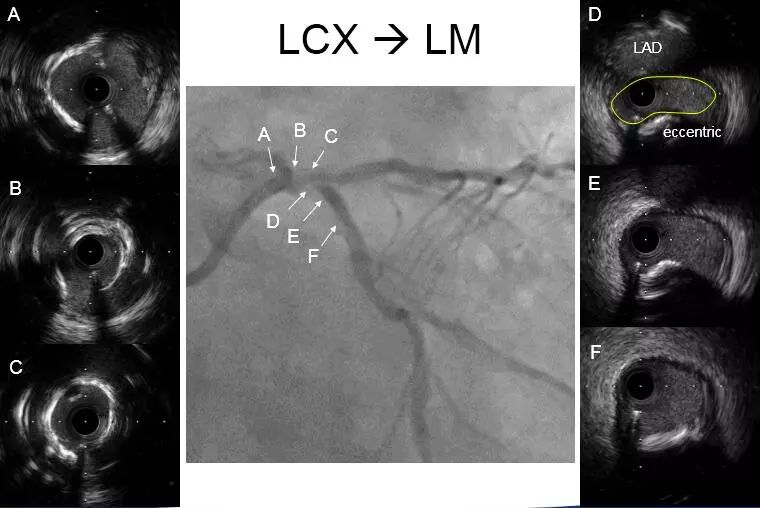
Setp 6: LAD→LM, Post stenting.
Final Angio:


Summary
1.Rotational atherectomy is necessary for severe calcified lesion.
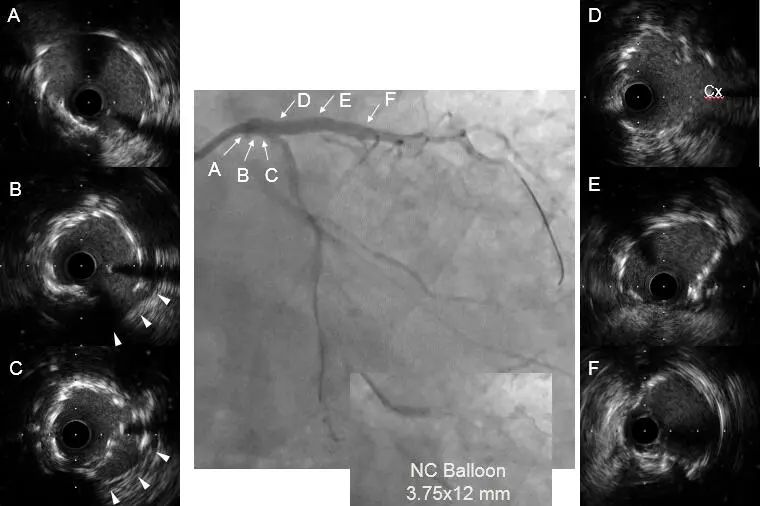
2.IVUS could provide valuable information: Pre-evaluation sometimes not available, Post-evaluation usually more important for lesion preparation and stent optimization.
3.Knowing not only what we can do, but also what we can NOT do, and where we should stop.
二维码(扫一扫即可分享)










