背景:在大和巨大型听神经瘤患者中,想看清内听道开口非常困难,甚至是不可能的。
目的:通过描述与分析TÜbingen线与内听道的关系,说明TÜbingen线是可用于定位内听道的硬膜标志线。
方法:十个尸头用于本项研究。从2004-2009年,第一作者在300例听神经瘤患者中使用TÜbingen线作为辨认内听道的标志线。首先确定内耳门区几个笔直的硬膜反折,之后反折水平向上延伸并逐渐终止,该处硬膜与骨面紧密粘连,表面光滑无折叠。
结果:在所有尸头标本和298例听神经瘤手术中均能确认TÜbingen线。在尸头标本中,磨除TÜbingen线上方的骨质即可定位内听道,同样在手术中发现TÜbingen线也有助于定位内听道。
结论:TÜbingen线是一个简单、稳定、安全的方法,来定位内听道在颞骨后部的表面投影。
关键词:解剖,内听道,乙状窦后入路,听神经瘤
听神经瘤占颅内肿瘤的6-8%,占桥小脑角区肿瘤的80-90%。由于技术的进步,近十年来大部分病例可以做到全切肿瘤而颅神经功能保护良好。
乙状窦后入路有利于面听神经功能的保护,在此入路中,如何磨除内听道后壁是保留神经功能的关键。
在大型和巨大型听神经瘤中,想在颞骨后部表面看到内听道开口是不可能的。
尽管有许多文献描述在乙状窦后入路中如何磨除内听道后壁的技巧,其中一些描述如何避免打开内耳结构的安全磨除方法,但均未从手术解剖学角度去找一条定位内听道后壁的标志线。
第一作者在经乙状窦后入路行听神经瘤切除术中,在磨除内听道后壁时,发现颞骨岩部一个硬膜标志线与内听道下极关系密切,这条线被称为TÜbingen线。
本文描述TÜbingen线并揭示其与内听道的关系,有助于在乙状窦后入路手术过程中磨除内听道后壁。
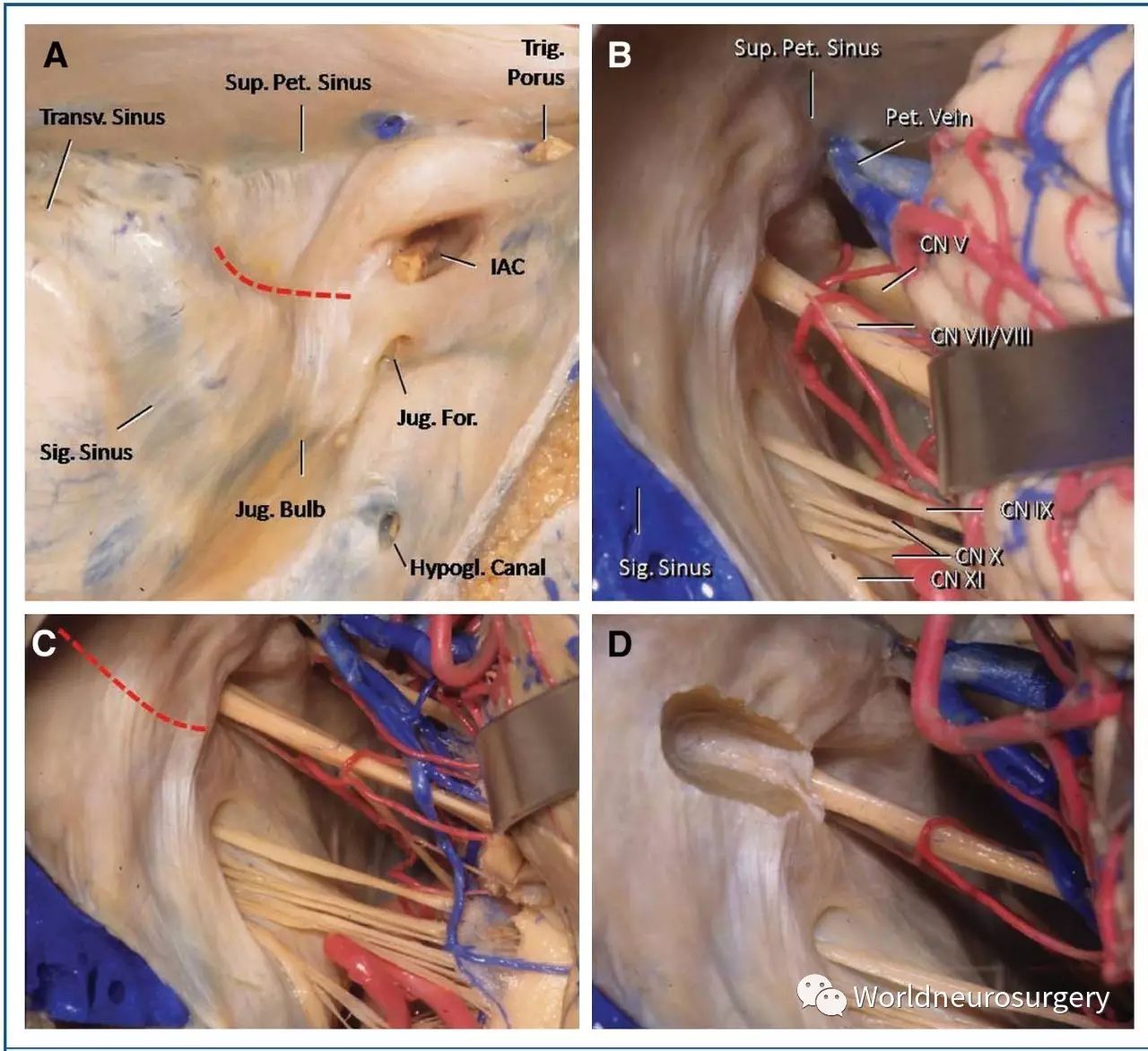
FIGURE 1. Cadaveric pictures. A, medial to lateral view into the left posterior fossa. The posterior surface of the temporal bone is
surrounded by venous sinus: the superior petrosal sinus, above, the junction of transverse and lateral portion of sigmoid sinus, laterally, the junction of medial portion of the sigmoid sinus and jugular bulb, inferiorly, and the basilar sinus, medially (not shown). The internal acoustic meatus is located between the trigeminal porus superomedially and the jugular foramen,
inferolaterally. The Tu¨bingen line (dotted red line) connects the ending points of the dural folds spanning the area comprised
between the jugular foramen and the medial part of the sigmoid sinus inferiorly and extending cranially for 5 to 7 mm. This dural landmark points out the inferior limit of the internal acoustic meatus. B, retrosigmoid view into the left posterior fossa. Observe the presence of several, delicate dural folds around the area of the vestibular aqueduct. Following these folds upward reaches a linear level where the folds end and the dura tightly adheres to the bony surface. C, magnified view of B. The Tu¨bingen line has been highlighted in red. D, same specimen shown in C. The internal acoustic meatus has been drilled to expose the dura in the canal, protecting the meatal portion of VII/VIII nerves. Tu¨bingen line is a useful landmark for the lower limit of the internal
acoustic meatus. CN, cranial nerve; For., foramen; Hypogl., hypoglossal; IAC, internal acoustic meatus; Jug., jugular; Pet.,
petrosal; Transv., transverse; Trig., trigeminal; Sup., superior.
图1: 尸头照片。A、从内侧至外侧看左后颅窝。颞骨后表面被静脉窦围绕:上有岩上窦,侧方为横窦与乙状窦结合部,下方为乙状窦与颈静脉球结合部,内侧为基底窦(未显示)。内听道位于内上方的三叉神经孔和下外侧的颈静脉孔之间。TÜbingen线(红色虚线)是颈静脉孔与下方乙状窦远端区域硬膜反折的终点之连线,向头部延伸5-7mm。硬膜标志线提示了内耳道下极。B、从乙状窦后入路看左颅后窝。观察内耳门区几个细微的硬脑膜反折。顺着这些反折向上反折终止并形成线形,该处硬膜与颅骨表面紧密粘连。C、B的放大图。红色高亮显示TÜbingen线。D,与C同一标本。内听道已磨除,暴露内听道硬脑膜。面听神经保护良好。TÜbingen线可作为内听道下极的标志线。CN,颅神经;For.,颈静脉孔;Hypogl.,舌下神经;IAC,内听道;Jug.,颈;Pet.,岩;Transv.,横窦向;Trig.,三叉;Sup.,上方。
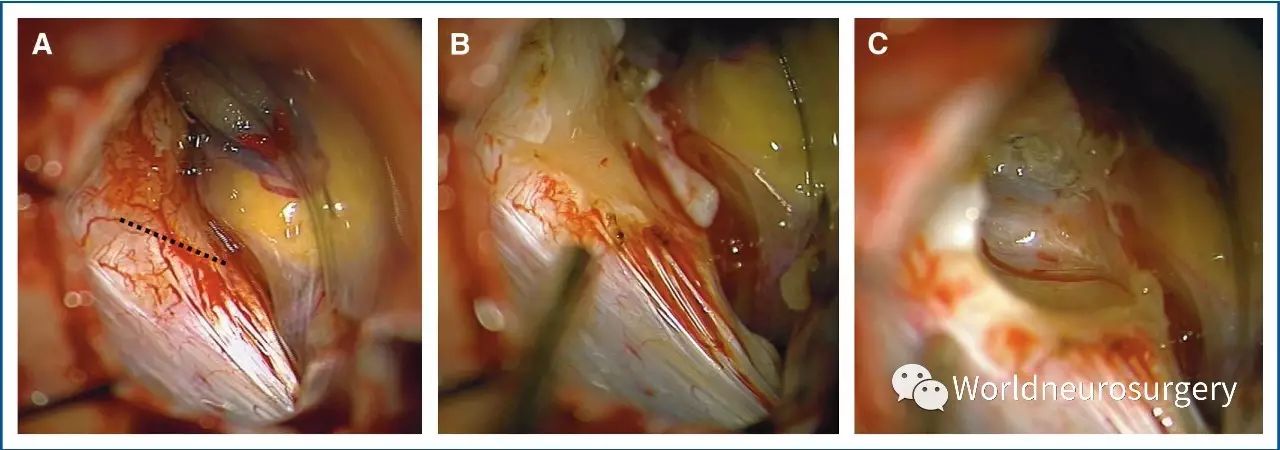
FIGURE 2. Surgical pictures. A, retrosigmoid view into the left posterior fossa. The Tu¨bingen line has been highlighted in dotted black line. B, the dura covering the posterior
wall of the IAC has been removed in order to start the drilling. Observe that the inferior limit of the drilling is at the level of the Tu¨bingen line. C, the posterior wall of the IAC
was already drilled. Note that the Tu¨bingen line corresponds with the inferior limit (floor) of the IAC.
图2。手术图片。A、左后颅窝乙状窦后入路视图。TÜbingen线已用黑色虚线显示。B,内耳门后壁的硬脑膜已经剥离,准备磨除骨质。磨除下限位于TÜbingen线水平。C、内耳门后壁已经磨除。注意TÜbingen线与IAC下壁的关系。
结果
确定TÜbingen线
The Tu¨bingen line was easily identified in all temporal bones
studied and in all 300 patients operated on, with the exception
of 2 cases (, 1%). The dural folds guiding its identification
spanned the area between the jugular foramen and distal part of
the sigmoid sinus inferiorly and extended 5 to 7 mm cranially.
The line connecting the ending points of the dural folds sloped
upward from medial to lateral, forming a slightly upward
concavity or rather an ascending path (Figures 1A–1C, 2A
and 2B).
在所有的颞骨标本和300例手术患者(除2例之外(1%))中均可以确认TÜbingen线。位于颈静脉孔与下方的乙状窦远端之间区域的硬膜反折是确定TÜbingen线的向导,TÜbingen线由硬膜反折的止点由内向外斜向上,沿颅骨面延伸5-7mm,行程上端稍弯曲(图1a–1c,2a和2b)。
In 2 cases the Tu¨bingen line was not useful because the anteroinferior
cerebellar artery was located and also attached in the
dura over the posterior wall of the internal auditory canal; thus, in
both patients it was impossible to recognize the line, because the
line was hidden by the artery.
2例的TÜbingen线无法确定,主要是因为小脑前下动脉与内听道后壁硬膜粘连,该线位于小脑前下动脉下方故无法辨认。
内听道与TÜbingen线之间的关系
Removal of the bone just above the Tu¨bingen line located the
IAC in all temporal bone specimens studied (Figure 1D),
demonstrating that this landmark consistently lead to the inferior
limit of the IAC. Similarly, the analysis of the relationship between
the Tu¨bingen line and the IAC in surgical cases showed
that the Tu¨bingen line helped locate the IAC in all cases and
consistently marked its inferior limit (Figure 2B and 2C).
在所有颅骨标本中磨除位于TÜbingen线上方内听道处的颅骨(图1d),证实这条标志线与内听道下缘一致。同样分析手术病例,TÜbingen线也有助于确定内听道的下沿极(图2b和2c)。
讨论
The incidence of giant tumors among all cases of VS has been
estimated to be up to 2% in Western countries,11 but in developing
countries, as in skull base referring centers, they are seen
with a significantly higher incidence.2 The final goal of VS
surgery is to achieve complete microsurgical tumor resection with
functional preservation of facial and cochlear nerves.12
西方国家巨大听神经瘤发病率占所有听神经瘤的2%,但在发展中国家的颅底治疗中心发生率更高。听神经瘤的手术终极目标是肿瘤全切除而面听神经功能保护完好。
Removal of the posterior wall of the IAC is an essential step in
VS surgery via the retrosigmoid approach.13 Of the many factors
influencing hearing preservation, inadvertent fenestration of the
labyrinth, during IAC exposure, is one of the more common and
perhaps one of the more avoidable complications.14 Thus, different
guides to work out the amount of drilling needed at the
distal most lateral end of the canal that may be performed to
maximize exposure while preserving inner ear structures—
specifically, the posterior semicircular canal, vestibule, and
common crus—have been advised by a number of authors.3-10
Tatagiba et al14 and Yokoyama et al15 attempted to estimate the
preoperative risk of opening inner ear structures via the retrosigmoid
approach by introducing the sigmoid-fundus line.13
Other authors have stated that the predictive value of this anatomical
line is limited, and that the labyrinth is in danger
whenever exposure of the fundus is attempted.3,16
经乙状窦后入路切除听神经瘤需要磨除内听道后壁。在诸多影响听力的因素中,磨除后壁过程中的迷路开放是比较常见和严重的并发症。为了更好地保护内耳结构——譬如后半规管、前庭神经和总脚,有各种各样的指导方法用于控制内听道外极的磨除程度。Tatagiba等与Yokoyama等曾用乙状窦基底线(sigmoid-fundus line)预估在乙状窦后入路过程中内耳结构开放的危险度。另有人认为这条解剖线的预测作用有限,只要暴露基底,就有可能使内耳结构受到损伤。
In cases of large tumors, the medial end of the canal can also
offer difficulties. Large tumors typically hide the IAC opening
and might require tumor displacement to locate the IAC. This
maneuver usually causes bleeding at the dural-tumor interface.
The resulting clots may obliterate the surgical field, and continued
bleeding might require bipolar coagulation, risking the
nearby cranial nerves.
在大型听神经瘤中,内听道内侧难以确认。为了确认内耳门,常常需要推移肿瘤,这样将导致肿瘤与硬膜表面出血,持续出血会模糊视野,需要使用双极,这样就可能导致边上的颅神经损伤。
Pillai et al17 proposed using frameless navigation based on
high-resolution computed tomographic scans and the aid of the
endoscope to locate and guide the opening of IAC. Samii et al13
studied the role of image-guided opening of the IAC via the
retrosigmoid route and concluded that this method is promising
but still limited. Thus, opening of the IAC via the retrosigmoid
route remains today based mainly on careful analysis of preoperative
computed tomographic findings and the personal experience
of the surgeon.13
Pillai等提出使用基于高分辨率CT无框架导航和内镜辅助下定位和开放内听道。Samii等研究了影像导航在乙状窦后入路磨除内听道的作用后认为此方法可行但作用有限。因此,至今为止,在乙状窦后入路中开放内听道主要是基于术前对CT影像的仔细研究与术者个人的经验。
Before surgery, all patients had a CT scan to analyze, among
other surgical details, the position of the jugular bulb. In those
cases in which the jugular bulb was diagnosed as high, the
Tu¨bingen line was extremely useful during surgery, because the
drilling was started 3 to 5 mm above the line, avoiding the
possibility of damaging that highly situated jugular bulb. To
avoid a postoperative CSF fistula through the middle ear, in all
patients of this series, after the tumor was completely removed,
a piece of muscle and a bit of fibrin glue were put in the internal
auditory canal.
术前所有的患者均要进行头颅CT扫描,同时可以定位颈静脉球。在高位颈静脉球患者中,TÜbingen线非常有用,因为在该线上方3-5mm磨除骨质可以避免损伤高位颈静脉球。为了避免通过内耳产生的术后脑脊液漏,在所有手术患者中,均使用一片肌肉和纤维蛋白胶封闭内听道。
结论:
The Tu¨bingen line is an easy, consistent, and safe method to
locate the projection of the IAC along the posterior surface of the
temporal bone and to guide the initial drilling of the IAC in large
VS tumors.
TÜbingen线是一个简单、稳定、安全的方法,来定位内听道在颞骨后部的表面投影。
原著作者: Aaron Cohen
编译者:黄传平,中国人民解放军第421医院,神经外科,大病区主任,主任医师。
审校:澳门科大医院,神经外科,谭林琼教授。
RHOTON系列论文编译
鲜为人知的RHOTON实验室
显微入路到环池区域:解剖和定性研究
微血管减压术中的显微外科解剖
经小脑-脑干裂的解剖和手术入路-上
经小脑-脑干裂的解剖和手术入路-中
经小脑-脑干裂的解剖和手术入路-下
鞍膈开口大小预测垂体瘤的生长方向
儿童脑干肿瘤的手术治疗
前额骨膜瓣如何分离才能使颅底重建更可靠?
基于引流模式差异的岩上静脉和岩上窦分类法
内窥器在经蝶手术中的应用
巨大床突旁动脉瘤手术处理的细微差别
侧裂分离之大脑中动脉早期分支的显微解剖学
翼点入路:外科解剖,手术技术和理论基础(一)
显微外科切除侧脑室和三脑室肿瘤的手术入路(一)
翼点入路:外科解剖,手术技术和理论基础(二)
平台
手机微官网
全新排版,
识别二维码
体验



点击下方“
阅读原文
”查看手机微官网
↓↓↓




