乳腺钼靶筛查对于
普通
人群的作用存在争议。乳腺钼靶筛查虽然与乳腺癌死亡率减少相关,但是也与某些乳腺癌过度诊断相关。不过,过度诊断的程度尚不明确。美国各郡(又称县,是仅次于州的美国行政区划,例如洛杉矶县下辖88个市,拥有近1千万人口,首府为洛杉矶市,与中国的市辖县有所不同)筛查率相差很大,为调查筛查效果提供了天然机会。
2018年11月5日,国际抗癌联盟《国际癌症杂志》在线发表
美国哈佛大学、西雅图数据科学家与独立研究者
的研究报告,对1975~2009年美国各郡乳腺钼靶筛查率与乳腺癌诊断分类和结局进行了比较。
各郡的筛查率定义为年龄≥40岁女性过去2年接受乳腺钼靶检查≥1次的比例(范围34%~91%),分为两个时间段进行分析:
结果,观察到若干过度诊断迹象:
双重差分回归分析表明,
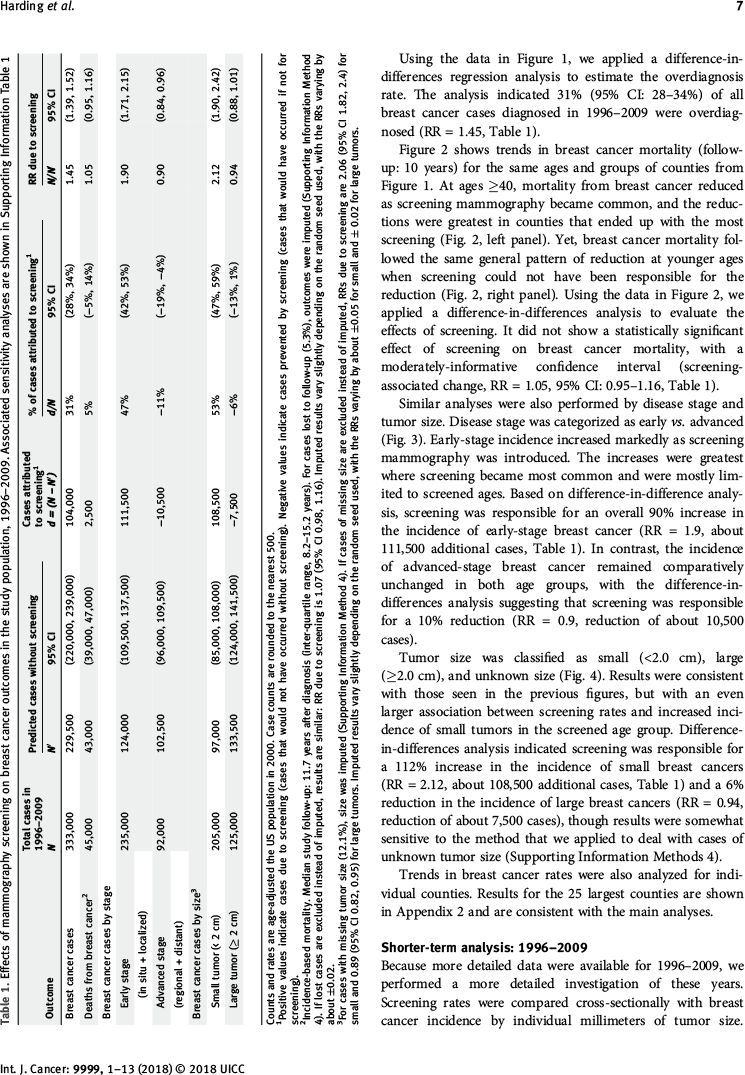
1996~2009年的乳腺癌过度诊断率为31%
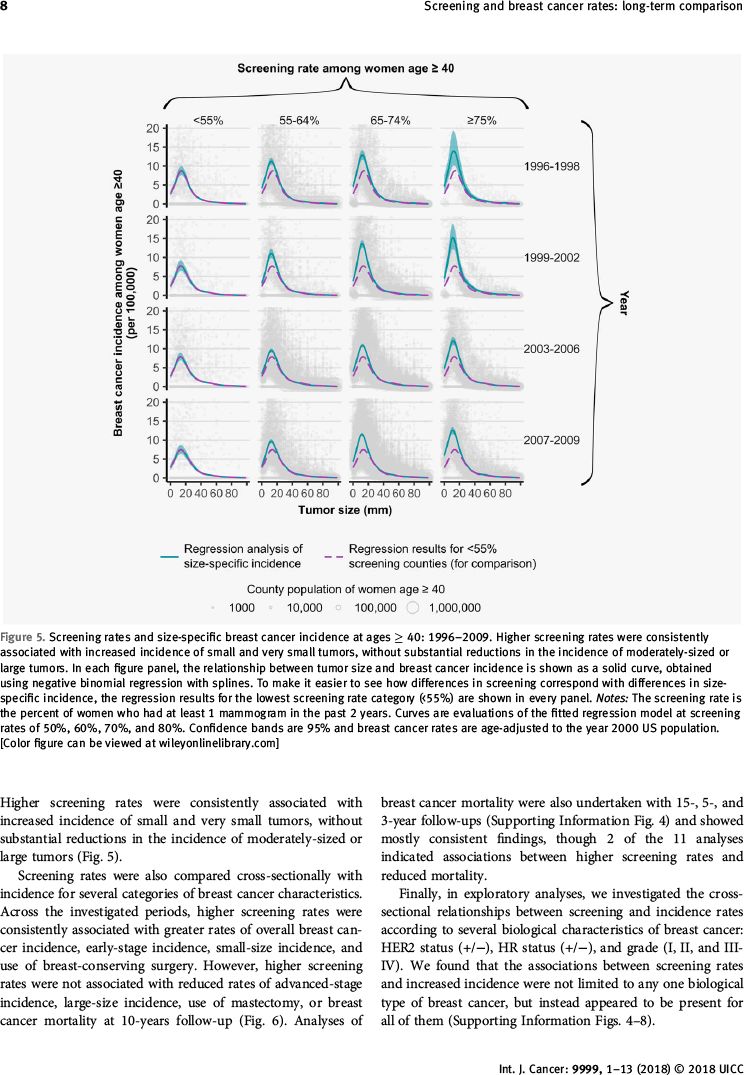
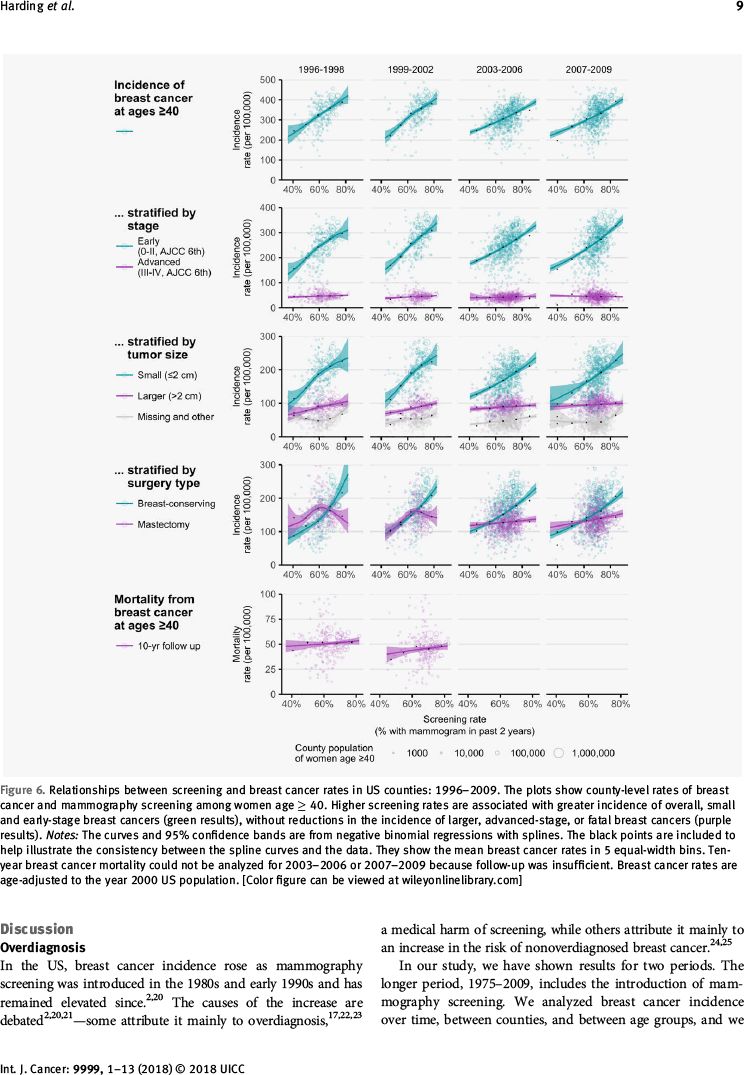
(95%置信区间:28%~34%)。筛查率与乳腺癌发病率成正比,无论激素受体状态、HER2状态、分级如何。
筛查与未筛查的各年龄组相比,1975~2009年乳腺癌死亡率减少相似。
因此,乳腺癌过度诊断的类似迹象遍及美国,但是过度诊断的肿瘤生物学特征并不明确。乳腺癌筛查减少死亡率的获益虽然可能存在并且相当可观,但是从整体人群水平无法检出。
Int J Cancer. 2018 Nov 5. [Epub ahead of print]
Long-term relationships between screening rates, breast cancer characteristics, and overdiagnosis in US counties, 1975-2009.
Harding C, Pompei F, Burmistrov D, Wilson R.
Data Scientist and Independent Researcher, Seattle, WA; Harvard University, Cambridge, MA; Exergen Corp, Watertown, MA; Worldpay, Lowell, MA.
What's new? Mammography screening is associated with reductions in breast cancer mortality and with some amount of breast cancer overdiagnosis. The extent of overdiagnosis, however, is uncertain. Here, the authors compared mammography screening and breast cancer rates in U.S. counties from 1975-2009, identifying multiple signs of widespread overdiagnosis, including elevations in breast cancer incidence as screening use climbed and leveling off of incidence as screening rates stabilized. Analyses suggest that overdiagnosis accounted for 31 percent of U.S. breast cancer cases between 1996 and 2009. Moreover, population-level analyses were unable to detect mortality benefits. No biological marker to identify overdiagnosis was found, however.
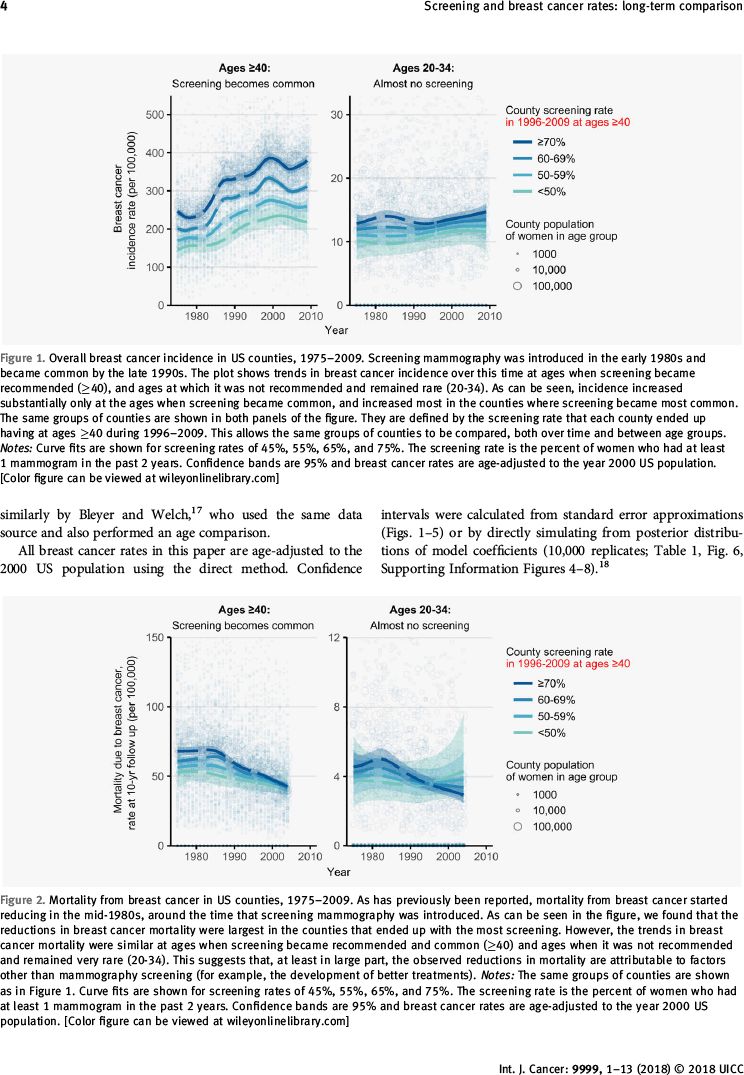
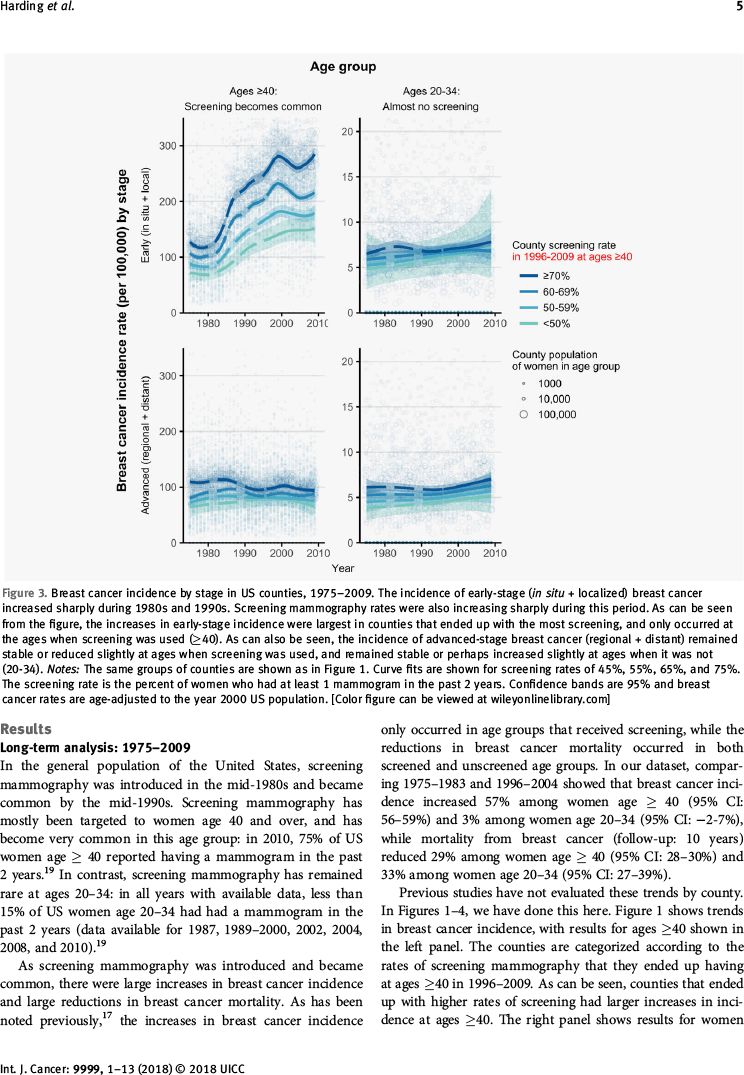
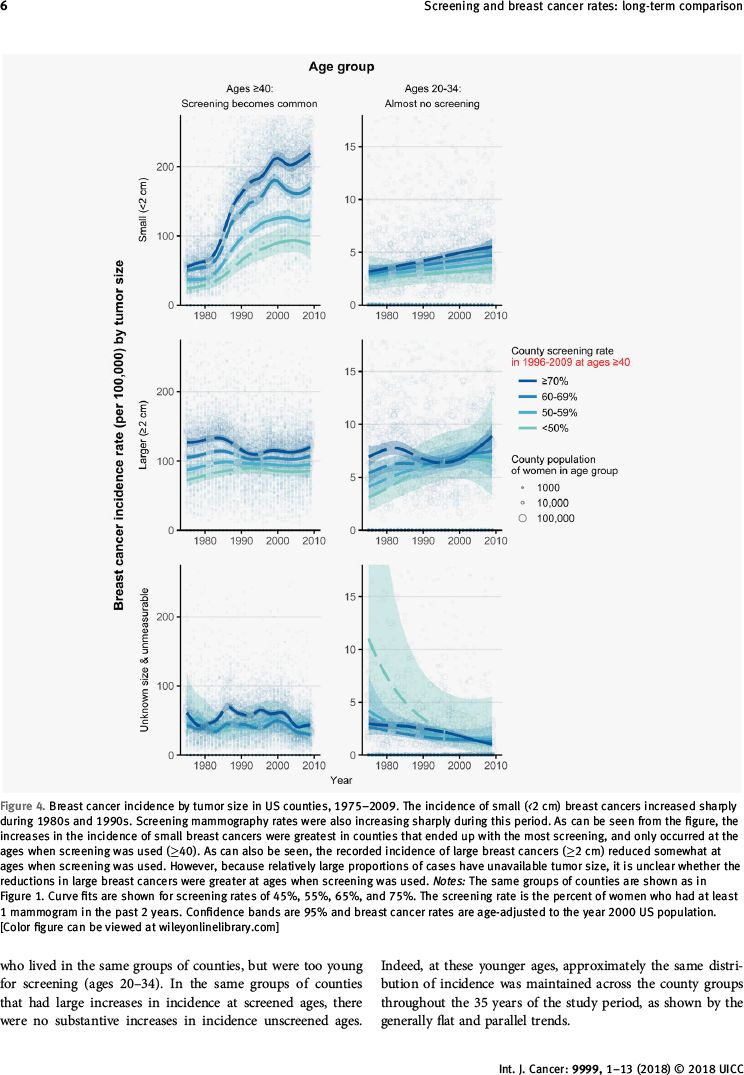
Effects of mammography screening in the general population are disputed. Screening rates differ greatly between US counties, providing a natural opportunity to investigate effects of screening. We compared mammography screening rates with the types and outcomes of breast cancers diagnosed in US counties. The county screening rate was defined as the proportion of women age ≥40 with ≥1 mammogram in the past 2 years (range, 34-91%). Two periods were analyzed: 1975-2009 (612,941 breast cancer cases, 195 counties) and 1996-2009 (645,057 cases, 211-547 counties). Multiple signs of overdiagnosis were observed: First, breast cancer incidence increased as screening became common. Second, incidence stopped increasing once screening rates stabilized. Third, the increases in incidence were limited to age groups receiving screening. Fourth, the increases were larger in counties where screening became more common. Fifth, the increases were limited to small and early-stage breast cancers (which are consistent with overdiagnosis). Sixth, compensatory reductions in large and advanced-stage breast cancers were much smaller than the increases. Difference-in-differences regression analysis suggested 31% (95% CI: 28-34%) of breast cancers diagnosed in 1996-2009 were overdiagnosed. Screening rates correlated with increased incidence for all hormone receptor statuses, HER2 statuses, and grades. Reductions in breast cancer mortality during 1975-2009 were similar in screened and unscreened age groups. Overall, we found repeated signs that breast cancer overdiagnosis is widespread in the US, but the biological nature of overdiagnosed tumors remains unclear. Mortality benefits of screening, though they may be present and substantial, could not be detected at the population level.
PMID
: 30264887
DOI
: 10.1002/ijc.31904







以下广告内容与本微信公众号无关





