本期目录:
1、基于16S核糖体RNA基因的一代测序和/或次代测序法在术前检测滑膜液来诊断关节假体周围感染上的临床应用
2、自动滑膜细胞计数对全髋关节置换术后不同无菌原因和假体周围病变情况的影响?
3、应用ICD-10编码骨水泥全髋关节置换术的精准性或缺陷分析
4、生物型全膝关节置换术的演变、当前适应证和结果
5、关节内注射治疗膝关节骨关节炎的疗效:随机对照试验的荟萃分析
6、全关节翻修术的趋势是否可持续?
7、高BMI患者的膝骨关节炎:骨科医生的角色
8、在髋关节发育不良中的“增生盂唇缘”和“新生盂唇脊”
9、股骨头软骨下骨折部位的分布与接触压力、年龄和髋臼结构有关
10、髋关节超声检查Graf 2a 随访结果
11、基于筛查策略的新生儿髋关节发育不良发生率和晚期检出率
12、晚期婴儿Blount病的治疗结果:胫骨内侧半平台抬高和干骺端截骨
13、髋臼周围截骨术治疗髋关节发育不良合并腓骨肌萎缩症患者的早期疗效
第一部分:关节置换及保膝相关文献
文献1
基于16S核糖体RNA基因的一代测序和/或次代测序法在术前检测滑膜液来诊断关节假体周围感染上的临床应用
译者 张轶超
摘要:
术前通过滑膜液培养来确定导致关节假体周围感染(PJI)患者的病原体常常是比较困难的。基于测序的方法是否有用于PJI病原体鉴定的潜力?如果有,哪种方法是理想的目前还不完全确定。本研究的目的是分析基于16S rRNA (rRNA)基因的PCR,随后采用一代测序和/或靶向宏基因组测序方法(tMGS)对滑液进行PJI诊断的准确性。进行了一项回顾性研究,分析了2020年8月至2021年5月在一个中心的滑液测试结果。本研究对髋关节、膝关节、肩关节和肘关节置换术患者进行了滑液抽吸,并进行了基于测序的方法和常规培养检查。研究共纳入154名受试者;非感染性关节置换术失败(NIAF) 118例,PJI 36例。基于测序方法诊断PJI的临床敏感性和特异性分别为69%和100%,常规培养诊断PJI的临床敏感性和特异性分别为72%和100% (P = 0.74)。两种方法联合使用比单独培养更敏感(83%)(P = 0.04)。基于测序的测试结果导致36名PJI受试者中4名(11%)患者的治疗方案改变。分别对19名受试者和6名受试者进行一代和次代测序进行微生物鉴定。当结合培养检查时,基于16S rRNA基因测序的方法比单独培养的敏感性更好,这表明其可以应用在滑液培养阴性PJI病例中。
重点:
假体周围关节感染(PJI)是关节置换术中一种可怕的并发症。感染性病原体的无创鉴定传统上仅限于基于培养的滑液检测,其敏感性较差。一代和次代测序(NGS)可用于PJI病例的滑液检测,但常规实践经验很少。当一代测序失败或可能失败时,我们使用靶向宏基因组测序方法对标本滑液进行常规检测。本研究的目的是分析该方法诊断PJI的性能,并将其与滑液培养的方法进行比较。总体而言,基于测序的方法在诊断PJI方面并不优于培养,但在一些培养阴性的样本中能够检测出阳性结果。
Clinical Use of a 16S Ribosomal RNA Gene-Based Sanger and/or Next Generation Sequencing Assay to Test Preoperative Synovial Fluid for Periprosthetic Joint Infection Diagnosis
Preoperative pathogen identification in patients with periprosthetic joint infection (PJI) is typically limited to synovial fluid culture. Whether sequencing-based approaches are of potential use in identification of pathogens in PJI, and if so which approach is ideal, is incompletely defined. The objective of the study was to analyze the accuracy of a 16S rRNA (rRNA) gene-based PCR followed by Sanger sequencing and/or targeted metagenomic sequencing approach (tMGS) performed on synovial fluid for PJI diagnosis. A retrospective study was conducted, analyzing synovial fluids tested between August 2020 and May 2021 at a single center. Subjects with hip, knee, shoulder, and elbow arthroplasties who had synovial fluid aspirated and clinically subjected to sequence-based testing and conventional culture were studied. A total of 154 subjects were included in the study; 118 had noninfectious arthroplasty failure (NIAF), while 36 had PJI. Clinical sensitivity and specificity for diagnosis of PJI were 69% and 100%, respectively, for the sequencing-based approach and 72% and 100%, respectively, for conventional culture (P = 0.74). The combination of both tests was more sensitive (83%) than culture alone (P = 0.04). Results of sequencing-based testing led to changes in treatment in four of 36 (11%) PJI subjects. Microbial identification was achieved using Sanger and next generation sequencing in 19 and 6 subjects, respectively. When combined with culture, the described 16S rRNA gene sequencing-based approach increased sensitivity compared to culture alone, suggesting its potential use in the diagnosis of PJI when synovial fluid culture is negative.
IMPORTANCE
Periprosthetic joint infection (PJI) is a dreadful complication of joint replacement. Noninvasive identification of infectious pathogens has been traditionnally limited to culture-based testing of synovial fluid which has poor sensitivity. Sanger and Next-generation sequencing (NGS) may be used for synovial fluid testing in PJI, but experience in routine practice is sparse. We used a targeted metagenomic sequencing approach for routine testing of synovial fluid involving NGS when Sanger sequencing had failed or was likely to fail. The objective of this study was to analyze the approach's performance for diagnosis of PJI in comparison to culture for testing synovial fluid.
Overall, the sequencing-based approach was not superior to culture for diagnosis of PJI, but yielded positive results in some culture-negative samples.
文献出处:
Flurin L, Hemenway JJ, Fisher CR, Vaillant JJ, Azad M, Wolf MJ, Greenwood-Quaintance KE, Abdel MP, Patel R. Clinical Use of a 16S Ribosomal RNA Gene-Based Sanger and/or Next Generation Sequencing Assay to Test Preoperative Synovial Fluid for Periprosthetic Joint Infection Diagnosis. mBio. 2022 Dec 20;13(6):e0132222. doi: 10.1128/mbio.01322-22. Epub 2022 Nov 10. PMID: 36354331; PMCID: PMC9765659.
文献2
自动滑膜细胞计数对全髋关节置换术后不同无菌原因和假体周围病变情况的影响?
译者 马云青
背景:
研究表明,评估髋关节置换术后患者可能存在的关节假体周围感染时,关节液细胞计数可能会高估白细胞(WBC)计数,导致假阳性结果。然而,WBC计数升高的很多患者关节置换术后并未感染,但存在各种无菌性问题(包括但不限于金属磨损,聚乙烯磨损和复发性脱位),这些患者与PJI患者白细胞升高的区别尚未得到充分解决。此外,在这种情况下,自动分析仪评估的多形核细胞百分比(PMN%)也缺乏进一步的研究。
研究目的:
在无菌性翻修的不同适应症和不同的髋关节假体周围病理结果的背景下,问题:(1)关节液WBC计数水平是多少,以及高于2018年国际共识会议(ICM)确定的值(3000个细胞/μL)的数值的比例是多少?(2)关节液中性粒细胞百分比水平为多少,高于2018年ICM确定的(70%)比例为多少?
方法:
作者回顾性研究了2015年1月至2017年12月在三级转诊关节置换中心接受无菌性THA翻修的患者术前滑液细胞计数并进行分析。排除了部分患者(排除主要包括15%[1306例中的197例]缺失数据的患者和12%[1306例中的155例]穿刺抽液获得的关节液不足的患者),共有702例接受无菌原因翻修THA的患者纳入最终的分析。患者平均随访46±11个月,没有患者因PJI再次翻修,即这些髋关节确实没有PJI。使用自动分析仪进行细胞计数分析。临床表现,术前影像学检查和手术报告——由可用的组织学结果证实——被用来确定诊断。考虑到2018年ICM的标准(WBC计数为3000个细胞/μL,PMN为70%),作者评估了这些髋关节,以了解根据这种诊断值,其中哪些患者可能具有PJI。整个队列的平均白细胞计数为2120±2395个细胞/μL。整个队列的平均PMN%为36%±22%。
结果:
与无菌性松动和复发性脱位相比,聚乙烯磨损的平均白细胞计数最高(3817±3711细胞/μL;p<0.001)。在研究的假体周围条件中,磨损引起的滑膜炎的值最高(4464±3620个细胞/μL;p<0.001)。考虑到ICM的诊断值,在无菌翻修的适应症中,聚乙烯磨损显示WBC计数高于3000个细胞/μL的比例最高(60%[42/25];p<0.001)。在假体周围病变的情况下,磨损引起的滑膜炎在ICM诊断值以外的比例最高(60%[83/50];p<0.001)。无菌翻修的平均PMN%介于28%和44%之间,没有差异(p=0.12)。金属磨损导致翻修的患者的平均PMN%最高(45%±25%;p=0.007)。关于ICM的诊断值,金属病导致PMN%高于70%的患者比例最大(21%[47/10];p=0.003),磨损导致的滑膜炎为6%(83/5;p=0.42),骨溶解为3%(33/1;p=0.51)。无菌性松动、复发性脱位、聚乙烯磨损在无菌性翻修原因中所占比例均在70%以上,无明显差异。
结论:
使用自动细胞计数,作者发现WBC计数在THA无菌翻修的适应症中差异很大,并且由于无菌原因接受翻修的患者中有很高比例的WBC计数高于常用的3000个细胞/μL的诊断值。然而,PMN%在几种常见的无菌翻修THA适应症中受到的影响要小得多,这使得PMN%在使用自动分析仪测量抽液结果时更可靠,特别是在有聚乙烯磨损、金属对金属表面或疑似金属病的患者中,可以考虑手工计数技术。然而,在聚乙烯磨损的情况下使用自动分析仪观察到单独的WBC计数升高,不应该被认为强烈提示PJI,因为这一发现在感染的患者中并不常见。
What Is the Impact of Automated Synovial Cell Counting on Different Aseptic Causes and Periprosthetic Conditions Associated With Revision THA?
Background:
Studies have suggested that automated synovial cell counting may overestimate the white blood cell (WBC) count, resulting in false positive tests when evaluating patients for the possibility of periprosthetic joint infection (PJI) after THA. However, associations between WBC counts high enough to mimic PJI in patients whose arthroplasties are not infected but rather are experiencing a variety of aseptic problems-including but not limited to metallosis, polyethylene wear, and recurrent dislocation-have not, to our knowledge, been adequately addressed. In addition, there is a lack of analyses about the polymorphonuclear percentage (PMN%) when assessed by automated analyzers in this context.
Questions/purposes:
In the context of different indications for aseptic revision and different periprosthetic hip pathologic findings, we asked: (1) What were the synovial WBC count levels, and what proportion of values were above the 2018 International Consensus Meeting (ICM) cutoff (3000 cells/μL)? (2) What were the synovial PMN% levels, and what proportion of values were above the 2018 ICM (70%)?
Methods:
We retrospectively studied the preoperative cell count analyses of synovial fluid in patients who underwent revision THA for aseptic reasons at our tertiary referral arthroplasty center between January 2015 and December 2017. We considered all revisions performed on patients during that time potentially eligible, and after prespecified exclusions were applied (exclusions mainly included 15% [197 of 1306] sporadic missing data and 12% [155 of 1306] insufficient synovial fluid obtained in the aspirate), a total of 702 patients undergoing revision THA for aseptic reasons remained for the final analysis. As far as we know, no patients underwent re-revision for PJI at a mean follow-up of 46 ± 11 months, which tends to confirm our impression that indeed these hips did not have PJI. Cell count analyses were conducted using an automated analyzer. Clinical findings, preoperative radiographs, and surgical reports--confirmed by available histologic results--were used to establish diagnoses. We evaluated these hips considering the recommendations of the 2018 ICM (WBC count of 3000 cells/μL and PMN% of 70%) to see what proportion of them would have been characterized as likely having PJI on basis of those cutoff values. The mean WBC count for the entire cohort was 2120 ± 2395 cells/μL. The mean PMN% for the entire cohort was 36% ± 22%.
Results:
Compared with aseptic loosening and recurrent dislocation, polyethylene wear had the highest mean WBC count (3817 ± 3711 cells/μL; p < 0.001). Of the investigated periprosthetic conditions, wear-induced synovitis had the highest value (4464 ± 3620 cells/μL; p < 0.001). Considering the ICM threshold, polyethylene wear showed the highest proportion of WBC counts above 3000 cells/μL among the indications for aseptic revision (60% [25 of 42]; p < 0.001). Of the periprosthetic conditions, wear-induced synovitis showed the highest proportion beyond the ICM cutoff (60% [50 of 83]; p < 0.001). The mean PMN% for aseptic causes ranged between 28% and 44% without differences among them (p = 0.12). Patients with metallosis had the highest mean PMN% of the periprosthetic conditions investigated (45% ± 25%; p = 0.007). Regarding the ICM threshold, metallosis resulted in the largest proportion of patients with a PMN% above 70% (21% [10 of 47]; p = 0.003), and that for wear-induced synovitis was 6% (5 of 83; p = 0.42) and for osteolysis was 3% (1 of 33; p = 0.51). There were no differences among aseptic loosening, recurrent dislocation, and polyethylene wear in terms of the proportion above 70% among the aseptic revision causes.
Conclusion:
Using automated cell counting, we found that WBC counts differ widely across indications for aseptic revision THA, and a high proportion of patients who underwent revision THA for aseptic reasons had WBC counts above the commonly used threshold of 3000 cells/μL. However, the PMN% was much less affected in several common indications for aseptic revision THA, making this measure more reliable for interpreting aspiration results using an automated analyzer. Based on the data distributions we observed, manual counting techniques might be considered in particular among patients with polyethylene wear, metal-on-metal bearing surfaces, or suspected metallosis. However, an elevated WBC count alone, observed using an automated analyzer in the context of polyethylene wear, should not be considered to be strongly suggestive of PJI, since that finding occurred so commonly among patients without infection.
文献出处:
Abdelaziz H, Aljawabra A, Rossmann M, Tien CS, Citak M, Klatte TO, Gehrke T. What Is the Impact of Automated Synovial Cell Counting on Different Aseptic Causes and Periprosthetic Conditions Associated With Revision THA? Clin Orthop Relat Res. 2022 May 1;480(5):905-914. doi: 10.1097/CORR.0000000000002063. Epub 2021 Dec 1. PMID: 34851871; PMCID: PMC9007196.
文献3
应用ICD-10编码骨水泥全髋关节置换术的精准性或缺陷分析
译者 张蔷
背景:
国际疾病与健康分类系统,第十版,手术编码系统(ICD-10-PCS)于2015年在美国首次付诸应用。它的倡导者指出该分类诊断目录可以更加精准的覆盖各种类型的外科手术,提供包括术侧、关节部位和其他手术相关信息。然而,其他一些学者则担心编码数量的增加会使编码过于复杂,从而导致编码结果的精准性和一致性变差,进一步影响所有基于ICD-10-PCS编码的数据库资料和研究数据。我们希望确定ICD-10-PCS在鉴别骨水泥型初次全髋关节置换术(THA)方面的准确性。
方法:
我们回顾性入组了2015年至2020年间共四家医疗中心所有骨水泥型全髋关节置换病例。通过ICD-10-PCS分类系统辨识出骨水泥固定的病例。再通过浏览术后复查平片和手术记录分析其准确性,并将结果与美国关节登记中心(AJRR)的编码方法进行交叉比对。
结果:
共入组了552例骨水泥THA病例,其中452例(81.9%)被ICD-10-PCS准确标记为骨水泥型。各中心的准确比例分别为A中心 260例中的187例(72%)、B中心 185例中的158例(85%)、C中心 35例中的35例(100%)和D中心 72例中的72例(100%)。在三家医疗中心被成功标记的480例骨水泥THA病例中,403例(84%)被AJRR分类编码系统成功标记了骨水泥型(A,260中185[71%];B,185中185[100%];C,35中33[94%])。最后,在480例成功编码为骨水泥型的病例中,有317例(66%)被ICD-10-PCS和AJRR两种分类编码系统均准确编码。
结论:
我们的研究结果显示各家医疗中心之间存在着编码差异,而这种差异会导致AJRR或其他基于ICD-10-PCS编码系统的数据库产出不准确数据。我们在应用ICD-10分类编码系统评估手术细节时需要更加谨慎,以避免造成数据验证和解读过程中的误差。
Precision or Pitfall Evaluating the Accuracy of ICD-10 Coding for Cemented Total Hip Arthroplasty A Multicenter Study
Background:
The International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Procedure Coding System (ICD-10-PCS) was adopted in the U.S. in 2015. Proponents of the ICD-10-PCS have stated that its granularity allows for a more accurate representation of the types of procedures performed by including laterality, joint designation, and more detailed procedural data. However, other researchers have expressed concern that the increased number of codes adds further complexity that leads to inaccurate and inconsistent coding, rendering registry and research data based on ICD-10-PCS codes invalid and inaccurate. We aimed to determine the accuracy of the ICD-10-PCS for identifying cemented fixation in primary total hip arthroplasty (THA).
Methods:
We retrospectively reviewed all cemented primary THAs performed at 4 geographically diverse, academic medical centers between October 2015 and October 2020. Cemented fixation was identified from the ICD-10-PCS coding for each procedure. The accuracy of an ICD-10-PCS code relative to the surgical record was determined by postoperative radiograph and chart review, and cross-referencing with institution-level coding published by the American Joint Replacement Registry (AJRR) was also performed.
Results:
A total of 552 cemented THA cases were identified within the study period, of which 452 (81.9%) were correctly coded as cemented with the ICD-10-PCS. The proportion of cases that were correctly coded was 187 of 260 (72%) at Institution A, 158 of 185 (85%) at Institution B, 35 of 35 (100%) at Institution C, and 72 of 72 (100%) at Institution D. Of the 480 identified cemented THA cases at 3 of the 4 institutions, 403 (84%) were correctly reported as cemented to the AJRR (Institution A, 185 of 260 cases [71%]; Institution B, 185 of 185 [100%]; and Institution C, 33 of 35 [94%]). Lastly, of these 480 identified cemented THA cases, 317 (66%) were both correctly coded with the ICD-10-PCS and correctly reported as cemented to the AJRR.
Conclusions:
Our findings revealed existing discrepancies within multiple institutional data sets, which may lead to inaccurate reporting by the AJRR and other registries that rely on ICD-10-PCS coding. Caution should be exercised when utilizing ICD-10 procedural data to evaluate specific details from administrative claims databases as these inaccuracies present inherent challenges to data validity and interpretation.
文献4
生物型全膝关节置换术的演变、当前适应证和结果
译者 丁云鹏
全膝关节置换术(TKA)已经由整形外科医生进行了几十年,但生物型TKA直到最近才在关节成形术领域引起人们的兴趣。最初,早期的设计有多种并发症,特别是由于骨溶解和微动引起的无菌性松动。然而,改良显示出良好的效果和良好的生存率。在过去的几十年里,植入物设计以及植入物材料/涂层的变化有助于骨骼的生长和稳定性。此外,随着这些人群的增加,外科医生一直在对更年轻、更肥胖的患者进行TKA。在这些更具挑战性的人群中,与骨水泥型TKA相比,生物型TKA的良好结果可能是更好的选择,因为几项研究表明,年轻且BMI更高的患者存活率更高。此外,生物型TKA可能更具成本效益,这在当今的医疗环境中仍然是一个令人担忧的问题。总的来说,骨水泥和生物型TKA在现代取得了巨大的成果,但对于哪种植入物更好,仍存在争议。
The Evolution, Current Indications and Outcomes of Cementless Total Knee Arthroplasty
Total knee arthroplasty (TKA) has been performed by orthopedic surgeons for decades, but the cementless TKA has only recently gained much interest in the world of arthroplasty. Initially, early designs had multiple complications, particularly with aseptic loosening due to osteolysis and micromotion. However, modifications have shown good outcomes and excellent survivorship. Over the last several decades, changes in implant designs as well as implant materials/coatings have helped with bone in growth and stability. Furthermore, surgeons have been performing TKA in younger and more obese patients as these populations have been increasing. Good results from the cementless TKA compared to cemented TKA may be a better option in these more challenging populations, as several studies have shown greater survivorship in patients that are younger and have a greater BMI. Additionally, a cementless TKA may be more cost effective, which remains a concern in today’s healthcare environment. Overall, cemented and cementless TKA have great results in modern times and there is still a debate as to which implant is superior.
文献出处:
Maria T. Schwabe ,Charles P. Hannon,The Evolution, Current Indications and Outcomes of Cementless Total Knee Arthroplasty. J Clin Med. 2022 Nov; 11(22): 6608.
文献5
关节内注射治疗膝关节骨关节炎的疗效:随机对照试验的荟萃分析
译者 肖凯
目的:
骨关节炎是一种常见关节疾病,其特征是关节软骨的退行性变。关节内注射是重要非手术治疗方式,然而,关于患者的最佳注射药物存在争议。本研究的目的是对随机对照试验的文献进行荟萃分析,以确定是否存在最佳的用于膝关节骨关节炎治疗的关节内注射药物。
方法:
根据PRISMA指南进行文献检索。纳入了评估膝骨关节炎关节内注射的随机对照试验(RCTs)。提取数据,并分析了治疗后1、3、6和12个月时的VAS评分和WOMAC评分。采用频率学方法进行临床预后的比较。使用P-Score对治疗选项进行排名。
结果:
本研究纳入了79个RCTs,涉及8761名患者。评估的关节内注射包括自体调节血清(ACS)、骨髓抽吸浓缩物(BMAC)、肉毒毒素、糖皮质激素(CS)、透明质酸(HA)、间充质干细胞(MSC)、臭氧、生理盐水安慰剂、富血小板的血浆(PRP)、富含生长因子的血浆(PRGF)和脂肪组织血管基质(SVF)。在随访4-6周和3个月时,WOMAC评分最高的治疗方法是透明质酸和皮糖皮质激素(P-Score = 0.9500和8503)。在6个月随访时,WOMAC评分最高的治疗方法是PRP(P-Score = 0.7676)。在所有注射后时间节点VAS评分最高(P-Score=0.8631-0.9927)和12个月时Womac评分最高(P-Score = 0.9044)的治疗方法是SVF。
结论:
目前的证据表明,SVF注射在1年内能够使膝关节骨关节炎患者的疼痛和功能状况得到最大程度的改善。
The efficacy of intra-articular injections in the treatment of knee osteoarthritis: A network meta-analysis of randomized controlled trials
Purpose:
Osteoarthritis (OA) is a debilitating joint disease characterized by progressive loss of articular cartilage. Intra-articular injections are a mainstay of nonoperative treatment, however, there is controversy as to the optimal injectable for these patients. The purpose of the current study is to perform a network meta-analysis of the randomized control trials in the literature to ascertain whether there is a superior injectable nonoperative treatment for knee OA.
Methods:
The literature search was conducted based on the PRISMA guidelines. Randomized control trials (RCTs) evaluating intra-articular injectables in osteoarthritic knees were included. Data was extracted and Visual Analogue Scale (VAS) scores and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores, where available were analyzed at 1, 3, 6 and 12 months. Clinical outcomes were compared using a frequentist approach to network meta-analysis, with statistical analysis performed using R. The treatment options were ranked using the P-Score.
Results:
Seventy-nine RCTs with 8761 patients were included in this review. Intra-articular injectables evaluated included autologous conditioned serum (ACS), bone marrow aspirate concentrate (BMAC), botulinum toxin, corticosteroids (CS), hyaluronic acid (HA), mesenchymal stem cells (MSC), ozone, saline placebo, platelet-rich plasma (PRP), plasma rich in growth factor (PRGF), and stromal vascular fraction (SVF). At 4-6 weeks and 3 months of follow-up, the treatment with the highest P-Score for WOMAC score was high molecular weight (HMW) HA + CS [P-Score = 0.9500 and 8503, respectively]. At 6-months follow-up, the treatment with the highest P-Score for WOMAC score was PRP [P-Score = 0.7676]. At all post-injection time points, the treatment with the highest P-Score for VAS score [P-Score Range = 0.8631-9927] and Womac score at 12 Months [P-Score = 0.9044] was SVF.
Conclusions:
The current evidence shows that SVF injections result in the greatest improvement in pain and functional outcomes in patients with knee OA at up to 1 year of follow-up.
文献出处:
Anil U, Markus DH, Hurley ET, Manjunath AK, Alaia MJ, Campbell KA, Jazrawi LM, Strauss EJ. The efficacy of intra-articular injections in the treatment of knee osteoarthritis: A network meta-analysis of randomized controlled trials. Knee. 2021 Oct;32:173-182. doi: 10.1016/j.knee.2021.08.008. Epub 2021 Sep 6. PMID: 34500430.
文献6
全关节翻修术的趋势是否可持续?经通货膨胀调整后的住院医疗保险报销下降
译者 沈松坡
背景:
虽然在美国全关节翻修术(r-TJA)手术的负担在增加,但尚不清楚这些复杂病例的医疗资源分配是否跟上了步伐。本研究调查了医院层面对翻修TJA住院的报销趋势。
方法:
查询美国联邦医疗保险和医疗补助服务中心(CMS) 2014 - 2019年住院患者使用和支付公共使用档案,寻找翻修TJA的诊断相关组(DRG): DRG 467(合并并发症或共病的髋关节或膝关节翻修术)和DRG 468(无合并并发症或主要CC的髋关节或膝关节翻修术)。从2014年到2019年,医疗保险向170,808例翻修TJA住院收费,翻修TJA手术增加了3,121例(10.7%)。在以2019年美元为基准调整消费者价格指数后,进行多元线性混合模型回归分析。对这些DRGs进行了2014 - 2019年平均调整后的医疗保险支付和平均调整后的费用的协方差分析比较回归。
结果:
2014 - 2019年,DRG 467的平均调整后医疗保险支付减少了804.37美元(3.5%),而DRG 468的平均调整后医疗保险支付减少了647.33美元(3.6%)。在研究期间,与DRG 468相比,DRG 467的平均通货膨胀调整后的医疗保险支付率下降幅度更大(P =0 .02)。
结论:
DRGs 467和468的报销下降表明翻修TJA住院的动机降低。进一步的研究应评估当前医疗保险支付算法的有效性,并确定可能提供公平的医院级报销的修正。
Are Trends in Revision Total Joint Arthroplasty Sustainable? Declining Inflation-Adjusted Medicare Reimbursement for Hospitalizations
Background:
While the burden of revision total joint arthroplasty (TJA) procedures increases within the United States, it is unclear whether health care resource allocation for these complex cases has kept pace. This study examined the trends in hospital-level reimbursements for revision TJA hospitalizations. Methods: The Centers for Medicare and Medicaid Services (CMS) inpatient utilization and payment public use files from 2014 to 2019 were queried for diagnostic-related groups (DRGs) for revision TJA: DRG 467 (revision of hip or knee arthroplasty with complication or comorbidity [CC]) and DRG 468 (revision of hip or knee arthroplasty without CC or major CC). From 2014 to 2019, 170,808 revision TJA hospitalizations were billed to Medicare, and revision TJA procedures increased by 3,121 (10.7%). After adjusting to 2019 US dollars with the consumer price index, a multiple linear mixed-model regression analysis was performed. Analysis of covariance compared regressions from 2014 to 2019 for mean- adjusted Medicare payment and mean- adjusted charge were submitted for these DRGs.
Results:
Mean-adjusted average Medicare payment for DRG 467 decreased by $804.37 (3.5%) from 2014 to 2019, whereas, that for DRG 468 decreased by $647.33 (3.6%). The average inflation-adjusted Medicare payment for DRG 467 decreased at a greater rate during the study period, compared to that for DRG 468 (P 1⁄4 .02).
Conclusion:
The decline in reimbursement for DRGs 467 and 468 reveals decreasing incentives for revision TJA hospitalizations. Further research should assess the efficacy of current Medicare payment algorithms and identify modifications which may provide for fair hospital level reimbursements.
文献7
高BMI患者的膝骨关节炎:骨科医生的角色
译者 张峻
肥胖和下肢骨关节炎(OA)是世界范围内最常见的疾病之一,给卫生系统带来了越来越大的负担。两者之间的关系是复杂的。肥胖被认为是OA的一个危险因素,OA不利于减轻体重。全膝关节置换术(TKR)是一种应用广泛且有效的膝关节骨关节炎治疗方法。然而,高体重指数(BMI)会使手术复杂化,这导致一些外科医生拒绝对超过一定BMI的患者进行手术。骨科医生在帮助患者在准备TKR的过程中减肥方面发挥着重要作用。我们回顾了高BMI对出现症状性膝关节骨关节炎的影响,高BMI和TKR的并发症发生率,以及在OA存在的情况下减重的障碍,并指出了骨科医生可以在患者减重过程中为其提供支持的方面。我们回顾了证据,以确定基于患者的BMI拒绝患者进行TKR是否合理,并探讨了让高BMI患者参与的最有效方法,以提高他们进行无并发症TKR的可能性。
Knee Osteoarthritis in Patients With High BMI: The Role of an Orthopaedic Surgeon
Obesity and lower limb osteoarthritis (OA) are amongst the commonest conditions worldwide, with increasing burden on health systems. The relationship between the two is complex. Obesity is thought to be a risk factor for OA, and OA can hinder efforts to reduce weight. Total knee replacement (TKR) is a widely used and effective management for knee OA. However, high body mass index (BMI) can complicate the surgery, which leads to some surgeons denying this operation to patients above a certain BMI. Orthopaedic surgeons have an important part in helping patients lose weight in the process of preparing for their TKR. We review the effect of high BMI on developing symptomatic knee OA, the complication rate with high BMI and TKR and the obstacles to losing weight in the presence of OA and point to areas where the orthopaedic surgeon can find support for their patients during their journey to losing weight. We review the evidence to see whether denying patients a TKR based on their BMI is justified and look into the most effective way to engage high BMI patients to improve their chance of a complication-free TKR.
文献出处:
Hanoun A, Steele-Turner B, Chandratreya A. Knee Osteoarthritis in Patients With High BMI: The Role of an Orthopaedic Surgeon. Cureus. 2023 Nov 7;15(11):e48464. doi: 10.7759/cureus.48464. PMID: 38073938; PMCID: PMC10703516.
第二部分:保髋相关文献
文献1
在髋关节发育不良中的“增生盂唇缘”和“新生盂唇脊”
译者 罗殿中
“增生盂唇缘(limbus)”和“新生盂唇脊(neolimbus)”均为发育性髋关节脱位中反应性、病理性结构。对这些结构的深入理解对治疗髋关节发育不良(DDH)至关重要。但我们相信当前在对文献和矫形外科教科书的同行评议(peer-review)中,普遍存在对这些词汇的概念定义错误和应用不当。
“新生盂唇脊(neolimbus)”的最佳定义为:脱位的髋关节对髋臼外上区域的压力作用下,肥大的纤维软骨边缘。
“增生盂唇缘(limbus)”的最佳定义为:肥厚的盂唇,内含纤维和纤维软骨,是潜在阻挡对
发育不良髋关节行同心圆复位的结构。
我们对早期和当前的文献进行复习,试图明确“增生盂唇缘(limbus)”和“新生盂唇脊(neolimbus)”的概念和应用,概述并强调这些DDH相关的异常结构的重要性和针对性治疗。
(译者注:
感谢盛京医院小儿骨科李连永教授提供本文原文!翻译用词仅供参考。)
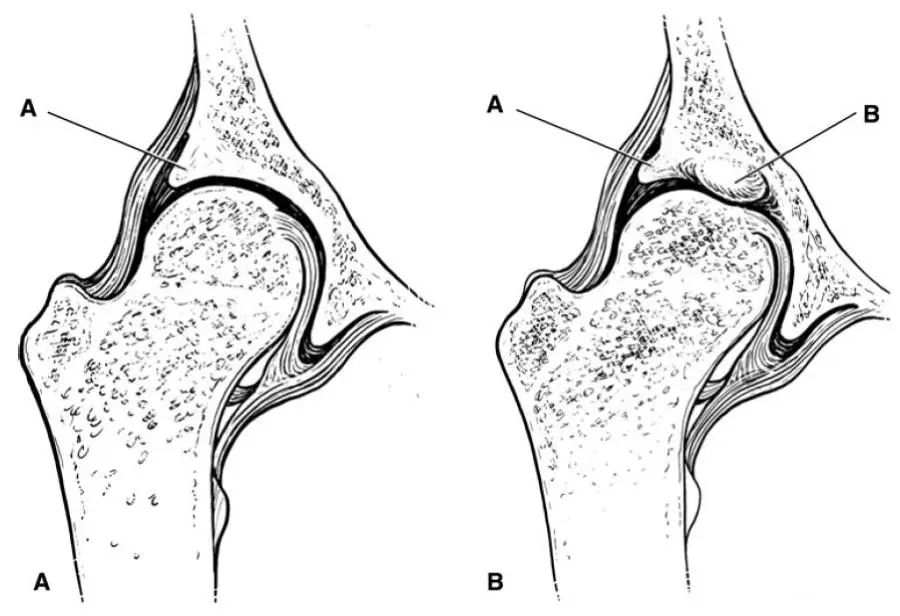
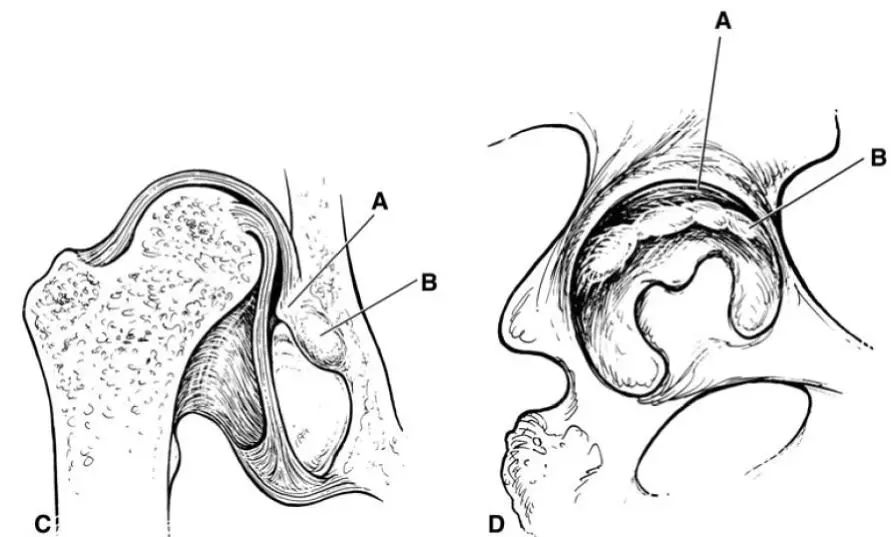
图1. A-D. A)在正常髋关节中,髋臼盂唇位于髋臼软骨边缘。B)在复位的发育不良髋关节中,肥大的盂唇,叫“增生盂唇缘limbus”[A],在髋臼软骨内有一肥厚的“脊”,成为“新生盂唇脊neolimbus”[B],在“增生盂唇缘limbus”的下方。C)在脱位的髋关节中,注意“增生盂唇缘limbus”[A]可阻挡复位,内翻或外翻;而“新生盂唇脊neolimbus”[B]不是阻挡复位的潜在因素,也不能内翻或外翻。D)侧面观察发育不良的髋臼,描绘出在“增生盂唇缘limbus”[A]的下方,“新生盂唇脊neolimbus”[B]从前向后的走行。
The limbus and the neolimbus in developmental dysplasia of the hip
The limbus and the neolimbus are both pathological lesions that form in response to a developmentally dislocated hip. An understanding of these structures is integral to treatment of developmental dysplasia of the hip (DDH). Yet, we believe the current peer-reviewed orthopaedic literature and orthopaedic textbooks commonly fail to correctly use or define these terms. The neolimbus is best defined as a hypertrophied ridge of fibrocartilage in the superolateral region of the acetabulum caused by pressure from the dislocated hip on this region. The limbus is the labrum that is hypertrophied with fibrous and fibrocartilaginous overgrowth, and is a potential block to concentric reduction of a dysplastic hip. We review the early and current literature in an attempt to clarify the use of the terms limbus and neolimbus and provide an overview of the importance and treatment of these abnormal structures associated with DDH.
文献出处:
Landa J, Benke M, Feldman DS. The limbus and the neolimbus in developmental dysplasia of the hip. Clin Orthop Relat Res. 2008 Apr;466(4):776-81. doi: 10.1007/s11999-008-0158-y. Epub 2008 Mar 12. PMID: 18335297; PMCID: PMC2504652.
文献2
股骨头软骨下骨折部位的分布与接触压力、年龄和髋臼结构有关
译者 张振东
目的:
非创伤性股骨头软骨下骨折常见于患有骨质疏松症和髋关节发育不良的老年患者。虽然这种损伤也可能发生在年轻人身上,或没有骨质疏松症的人群,但目前仍不清楚哪些人有此风险。本研究对年轻患者与中老年患者的髋臼结构和股骨头软骨下骨折部位进行了比较研究。
材料和方法:
共48 例非创伤性软骨下骨折患者,按年龄分为两组:年轻组(< 40 岁)和中老年组(≥ 40 岁)。髋关节发育不良和髋臼后倾分别定义为外侧中心边缘角<20°和骨盆正位X光片上交叉征阳性。通过测量T1冠状位磁共振图像上低信号强度带的边缘位置来评估骨折的部位和范围。并利用基于 CT 的有限元建模技术,对具有相同髋臼结构的未受影响的对侧髋部进行了评估,以确定年轻患者软骨下骨的应力分布。
结果:
48例股骨头不全骨折患者中,年轻患者 12 例,中老年患者36 例。41.7%的年轻患者表现为髋关节后倾,38.9%的中老年患者表现为髋关节发育不良。年轻患者的骨折部位多位于内/外侧,且骨折面积较大,而中老年患者的骨折则多位于外侧。两组中均有前上方骨折患者。
结论:
在年轻患者中常可观察到内外侧和前上方骨折,髋臼后倾会导致股骨头的异常应力分布,这表明髋臼后倾可能是年轻患者股骨头软骨下骨折的损伤机制之一。
Distribution of Femoral Head Subchondral Fracture Site Relates to Contact Pressures, Age, and Acetabular Structure
OBJECTIVE. Nontraumatic subchondral fracture of the femoral head (FH) is often seen in elderly patients with osteoporosis and acetabular dysplasia. Although this injury can also occur in young people, even those without osteoporosis, it remains unclear who is at risk. We examined the acetabular structure and sites of subchondral fracture of the FH in young patients compared with those in middle-aged and older patients. MATERIALS AND METHODS. Forty-eight hips with nontraumatic subchondral fracture of the FH were divided into two groups according to patient age: young (< 40 years) and middle-aged and older (≥ 40 years).
Dysplasia and retroversion were defined as a lateral center-edge angle of < 20° and crossover sign on anterosuperior radiographs, respectively. Locations and extents of fracture were evaluated by measuring the edge location of low-signal-intensity bands on coronal T1-weighted MR images. Stress distribution on subchondral bone in young patients was evaluated in contralateral unaffected hips with the same acetabular structure using finite element modeling based on CT. RESULTS. Twelve hips were in young patients and 36 were in middle-aged and older patients. Hips in young patients showed retroversion in 41.7%, whereas those in middle-aged and older patients had dysplasia in 38.9%. Young patients had larger mediolateral fractures; fractures in middle-aged and older patients were laterally located. Anterosuperior fractures were seen in both groups. Contact stress in patients with retroversion was mainly distributed on the mediolateral and superior sides but was concentrated laterally and superiorly in one patient with dysplasia. CONCLUSION. Mediolateral and anterosuperior fractures and stress distribution by retroversion were commonly observed in young patients, suggesting partial involvement of retroversion in the mechanism of injury of nontraumatic subchondral fractures of the FH in young patients.
文献出处:
Kubo Y, Motomura G, Utsunomiya T, Fujii M, Ikemura S, Sonoda K, Nakashima Y. Distribution of Femoral Head Subchondral Fracture Site Relates to Contact Pressures, Age, and Acetabular Structure. AJR Am J Roentgenol. 2020 Aug;215(2):448-457. doi: 10.2214/AJR.19.21895. Epub 2020 Jun 17. PMID: 32551906.
文献3
髋关节超声检查Graf 2a 随访结果
译者 任宁涛
目的:
评估Graf 2a型髋关节超声结果变差与DDH的危险因素、髋关节稳定性和初始超声分型之间的关系。
方法:
在2007年至2009年间接受髋关节超声检查的婴儿中,有3450人被纳入本研究。超声检查采用静态Graf技术和动态Harcke技术相结合。评估2a型髋关节的超声结果变差率,以及超声变差与DDH、髋关节不稳、未成熟侧别(右侧或左侧)、单侧和双侧不成熟髋关节的危险因素之间的关系。
结果:
529名婴儿中出现2a型髋关节(15.3%;780髋[11.3%])。其中,36名(6.8%;44髋[5.6%]),超声结果变差。36名中有25名(44髋中的32例)被诊断为2b型;另有6名(7髋)发育不良为2c型,3名(3髋)为D型,2名(2髋)为3型。不稳定、单侧2a型髋关节和相关中枢神经系统异常是2a型髋关节超声变差的独立预测因素。
结论:
2a型髋关节超声恶化率为5.6%;因此,超声随访是必要的。不稳定、中枢神经系统异常和单侧2a型髋关节被发现是超声结果变差的独立预测因素。我们的研究表明,有这些风险因素的病例应该更仔细地跟踪随访。
Follow-up sonographic results for Graf type 2A hips
Objectives:
The purpose of the study was to evaluate the association of sonographic worsening in type 2a hips with risk factors of developmental dysplasia of the hip, stability of the hip, and initial sonographic findings.
Methods:
Among infants who were referred for hip sonography between 2007 and 2009, 3450 were included in this study. Sonographic examinations were performed by combining the static Graf technique and the dynamic Harcke technique. The rate of sonographic worsening in type 2a hips and the relationship between sonographic worsening and risk factors for developmental dysplasia, instability of the hip, lateralization (right or left) of immaturity, and the presence of unilateral and bilateral immature hips were evaluated.
Results:
Type 2a hips were observed in 529 infants (15.3%; 780 hips [11.3%]). Of these, in 36 cases (6.8%; 44 hips [5.6%]), the sonographic results worsened. Twenty-five of these 36 cases (32 of 44 hips) were diagnosed as type 2 b; in others, the dysplasia worsened, and 6 cases (7 hips) were classified as type 2 c, 3 cases (3 hips) as type D, and 2 cases (2 hips) as type 3. Instability, unilateral type 2a hips, and associated central nervous system anomalies were found to be independent predictors of sonographic worsening in type 2a hips.
Conclusions:
Type 2a hips may worsen sonographically at a rate of 5.6%; hence, sonographic follow-up is needed. Instability, central nervous system anomalies, and unilateral type 2a hips were found to be independent predictors of sonographic worsening. Our study shows that cases with these risk factors should be followed more carefully.
文献出处:
Kosar P, Ergun E, Gökharman FD, Turgut AT, Kosar U. Follow-up sonographic results for Graf type 2A hips: association with risk factors for developmental dysplasia of the hip and instability. J Ultrasound Med. 2011 May;30(5):677-83. doi: 10.7863/jum.2011.30.5.677. PMID: 21527616.
文献4
基于筛查策略的新生儿髋关节发育不良发生率和晚期检出率:系统回顾和荟萃分析
译者 李勇
摘要:
尽管在随机临床试验中缺乏降低晚期检出率(年龄≥12周)的益处,但普遍超声筛查髋关节发育不良(DDH)已越来越受欢迎。









