前列腺癌作为男性发病率最高的肿瘤,而对于防治前列腺癌最好的办法就是通过筛查实现早诊早治,今天就让我们一起来听Elan给我们介绍前列腺筛查的相关知识吧~
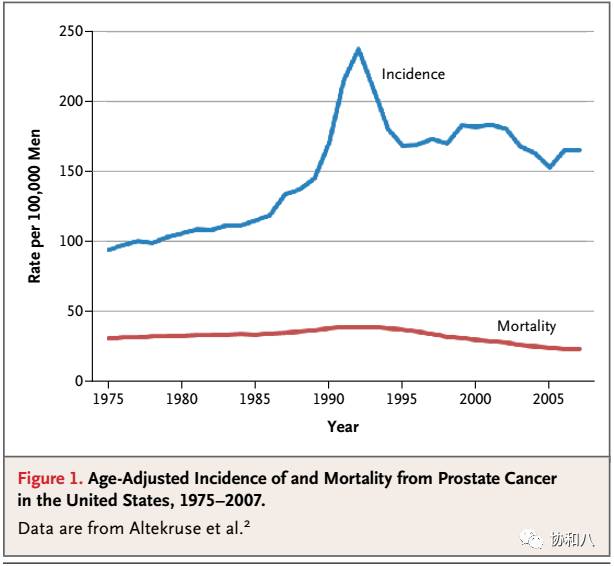
Prostate cancer is the most frequently diagnosed cancer in men in the United States. The age-adjusted incidence of prostate cancer is 165.8 cases per 100,000 men and mortality rates is 23.5 deaths per 100,000 men. The strongest risk factors for prostate cancer are older age and a positive family history.
(
New England Journal of Medicine, 2011, 365(21):2013-2019.
)
The rationale for screening is that early detection and treatment of asymptomatic cancers could extend life, as compared with treatment at the time of clinical diagnosis.
Digital rectal examination
For many years, the digital rectal examination was the primary screening test for prostate cancer. However, this test hasconsiderable interexaminer variability, and the majority of cancers detected by means of digital rectal examination are at an advanced stage.
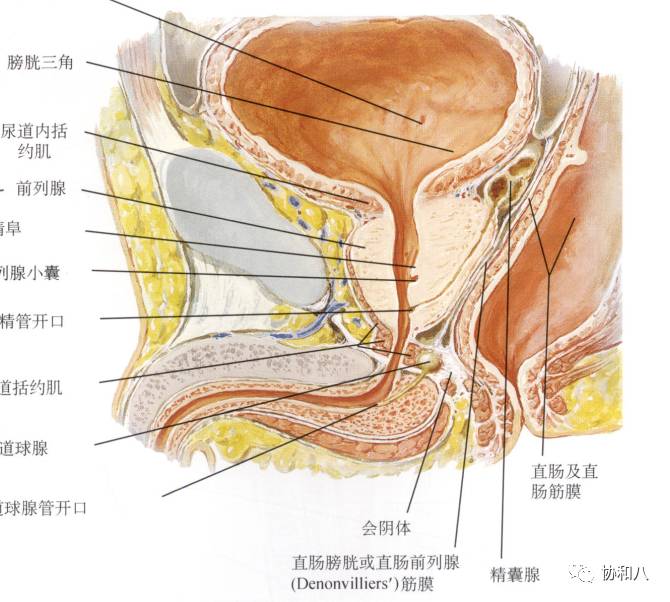
(奈特人体解剖彩色图谱)
PSA testing
After the introduction of
prostate-specific antigen (PSA) testing
, the lifetime risk of receiving a diagnosis of prostate cancer nearly doubled. The widespread use of PSA testing was based on its increased detection of early-stage cancer, but there was no evidence that testing reduced the risk of death from prostate cancer.
Chinese guideline for prostate cancer suggested that men over 50 years of age should undergone PSA testing and digital rectalexamination every year.
Initially,
PSA values above 4.0 ng
per milliliter were considered abnormal. Most abnormal PSA values are false-positive results that can be caused by benign prostatic hyperplasia, prostatitis or cystitis, ejaculation, perineal trauma, or the testing orsurgery in the urinary tract. Moreover, a normal PSA value does not rule out prostate cancer. As for PSA values between 4.0 to 10ng/mL, numerous approaches have been proposed to improve the diagnostic accuracy of the PSA test, including measuring PSA velocity, levels of free and protein-bound PSA and PSA density (PSAD).
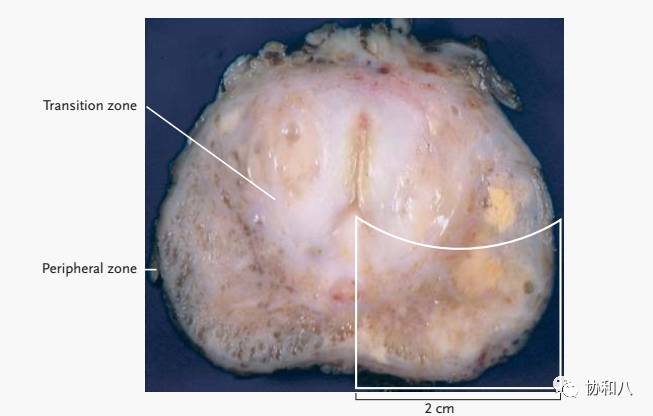
Biopsy
Prostate biopsy is the most reliable screening test. Abnormal PSA tests (that is, over 10ng/mL or 4~10ng/mL with abnormal free PSA or PSAD), abnormal imaging test or abnormal findings in digital rectalexamination leads to biopsies.
(
New England Journal of Medicine, 2003, 349(4):366.
)
Decisions about prostate-cancer screening should be based on the preferences of an informed patient. The man in the vignette should be engaged in a shared decision-making process that elicits his values and preferences for the potential consequences of testing.
Although articles on the initial trial results may have underestimated the potential benefit of screening with respect to prostate-cancer mortality, screening has not been shown to improve survival overall. In addition, the small absolute disease-specific survival benefit must be balanced against the potential harms of over diagnosis and complications of treatment, including urinary, sexual, and bowel dysfunction.
参考文献:
Hoffman R M. Screening for Prostate Cancer[J]. New England Journal of Medicine, 2011, 365(21):2013-2019.
Nelson W G, De Marzo A M, Isaacs W B. Prostate cancer[J]. New England Journal of Medicine, 2003, 349(4):366.
作者:
紫花苜蓿
配音:
ELAN
编辑:
毕日阳谷






